After witnessing the wonderful Wonca conference at Sheraton Grand, I thought Karnataka AFPI members would take a break. But it does not seem so. There was a meet and greet session held to welcome postgraduates in family medicine at Bangalore Baptist Hospital on May 24th, which was clubbed with a workshop on diabetes. This included interesting talks on management of diabetes in primary care, CGM devices, and research in primary care. Over 40 PGs and 20 to 30 faculty members across Karnataka attended, along with senior mentors like Dr. BC Rao and Dr[Col] Mohan Kubendra our national president.
Family medicine has been gaining recognition, with members being invited as keynote speakers in various health management inaugural programs like IIHMR Bangalore and media events like 5K run.
Members participated in MND [Motor Neuron Disease] meeting held at Arogya Soudha on 22nd June where importance of family medicine was highlighted to principal secretary Mr Harsh Gupta. The popularity of family medicine is being well-established in Karnataka, especially in Bengaluru and surrounding areas.
The evergreen and enthusiastic Karnataka state organizing team has decided to hold a state conference with the theme on women and child health on August 2nd and 3rd at St John medical college Auditorium. This includes workshops on emergencies in primary care, skill development, point-of-care ultrasound, and topics like adolescent health, cesarean sections, and lifestyle medicine. For this insightful conference Ms Padmasri and Dr C N Manjunath, Member of Parliament have kindly agreed to participate.
Before the conference, we had a webinar on occupational therapy and its relevance to primary care on July 3rd 2025.
There is also an upcoming webinar on newer versus conventional insulin with expert insights.
The Karnataka chapter organizing team has put in a lot of effort to make this conference meaningful and pertinent to day-to-day practice.
I request everyone across Karnataka and other states to participate and utilize the workshops, which are one of their kind. We also hope to see you all at the upcoming state conference.
Regards
Dr Sowmya B Ramesh
President AFPI K
Secretary's Letter
Dear Members,
Greetings from AFPI Karnataka!
It gives me immense pleasure to invite you to the 5th State Conference of AFPI Karnataka Chapter -- Family Medicine Update 2025, to be held on the 2nd and 3rd of August 2025 at Lecture Hall 1 Auditorium, St John's Medical College, Bangalore.
This year's theme, "Every Stage, Every Age: Family Medicine Transforming Women and Child Health," reflects our ongoing commitment to holistic, inclusive, and age-spanning care. The conference promises to be an enriching platform for academic exchange, skill enhancement, and networking for family physicians, academicians, trainees, and students.
Highlights of the Conference:
Hands-on clinical skill training and interactive workshops
Quiz and collage competition
Thought-provoking panel discussions
Recent updates on core and emerging topics in family medicine
Paper and poster presentations for knowledge sharing and showcasing research
We encourage all our members to register early and actively participate in the academic and extracurricular segments of the event. Your involvement will make the event truly representative of our vibrant family medicine community.
Please stay tuned for updates on registration details, abstract submissions, and event schedules. Let us come together to celebrate and strengthen our collective vision for comprehensive care through every stage of life.
Looking forward to your enthusiastic participation.
Warm regards,
Dr. Hemavathi D
General Secretary
Editor's Note
There is an often-heard complaint that patients once referred to a specialist are lost for the referring family doctor. When a patient is referred to a consultant in a hospital, it is likely that, that doctor will get tests done or send the patient to another doctor as both are available under one roof, especially so it there is urgency in doing so. While this is justifiable in some situations what is not justifiable is to ask the patient to see him once again for a follow up. In countries where a patient cannot see a consultant unless referred to by the primary care doctor and the patient so referred will remain on the roster of the primary care team, in countries where there is no such rule, it is a free for all, and patient is at liberty in not coming back to the primary care referring doctor.
Given this situation what can be done to see that the patient returns. First, one should write a note in which it should be made clear that the patient is referred back if no urgent tests are required or another consultant to come into the picture. This does not always work. Then the primary care doctor should call and ask what has happened to the patient sent for an opinion. This will make the consultant sit up and take notice. Another method is to tell the patient to call after seeing the consultant and discuss the advice given. Over the years a kind of network will be built up between the referring doctor, patients and consultants and cross referrals and so-called loss of patients get minimized.
B C Rao
AFPI Karnataka News
With the successful completion of WONCA SAR 2025, a consensus was arrived on holding the state conference in the first weekend of Aug 2025 (2nd and 3rd August), the various committees were formed and the works tarted vigorously.
Another landmark achievement was successful completion of Hematology course with more than 100 doctors coming out certified.
Meet and Greet session was held in partnership with Spice route on 24th May 2025 and official announcement was made for state conference and first registration done on the same day. Diabetes workshop was conducted and P G orientation took place.
Instead of celebrating Family doctor's day only on 19th may, the whole month was dedicated to create awareness about family doctors by creating chain of videos in social media with short clips of family physician's sharing this year's theme and how they achieve it.
A visit to Strand Lifesciences Lab was made by a group of doctors (Dr Jyotika Gupta, Dr Srividya Raghavendra, Dr Gowri C, Dr Supritha , Dr Madhumitha R) on 3rd June to understand the genomic testing and various futuristic approach to health care.
Dr Sowmya, President AFPI Karnataka, Dr Hemavathi Dasappa, secretary, AFPI Karnataka, Dr Anupama Nagaraj, Advisor, executive committee, Dr Amrutha JH, executive committee member, left no stone unturned, and took the extra effort to meet Honorable MP, Dr. C N Manjunath on 16th June and put forward the need to create openings for specially in Family Medicine for doctors in Govt setups.
Dr Sowmya B Ramesh , President, AFPI Karnataka and Dr Hemavathi Dasappa, Secretary, AFPI Karnataka, were invited to attend the workshop on Global Motor Neuron Disease on 21st June, conducted by Directorate of Health and Family Welfare, Govt of Karnataka and DR. Shyama Narang Foundation, where once again they reinforced the need of the hour -- "A good Family physician, a healthy community."
Dr Madhumitha
Not every swollen gland has TB's hand; a case series
Case 1
Case 2
28/F, home maker from Bangalore, Karnataka
44/F, home maker, from Kudappa, AP
Hx
Painless swelling in the right side of neck -3 w
High grade, intermittent, Fever- 3 w
Multiple small & large joint painful swelling-3 w
Significant unintentional Weight loss- 3 m
High grade, intermittent fever -- 2 d
Painless Swelling on the left side of neck -2 d
Past h/o- 6m ATT due to clinical TB lymphadenopathy
Ex
Pallor+
Left submandibular LN+ (multiple, matted, mobile, smooth surface, 3x5 cm)
Right supraclavicular LN (single, mobile, smooth, 2x2 cm) B/L pitting pedal edema
Systems: normal
MSK-tender, warm swellings of small & large joints with painful range of movements.
Pallor+
Single right upper jugular LN (smooth, mobile, nontender, 1x1.5cm)
Single left lower jugular LN (smooth, mobile, nontender, 1x1 cm), fine tremor of hand+
Systems: normal.
Ix
Parameters | Values
HB | 9.8
TLC (DC) | 1.92 (56/37/0.5/6.1/0)
ESR | 44 mm/hr
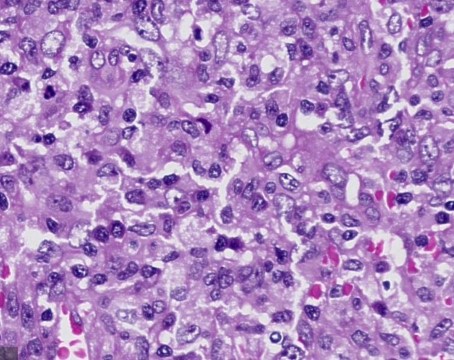
RF, Anti-CCP | <10,7 USG neck: Multiple enlarged LN (Ib,II-V) bilateral with loss of fatty hilum FNAC: Histiocytes aggregates with scanty necrosis. Biopsy: Histiocytosis with scanty necrosis
Reduced appetite -- 6 m
Significant unintentional weight loss -- 2 m
Low-grade, intermittent fever with chills and myalgia -- 2 w
High-grade intermittent evening fevers with chills- 10 d, Frontal dull aching headache -10
Progressive shortness of breath with no orthopnea-8 d
Ex
Pallor+,
Multiple B/L submandibular and upper jugular LN (mobile, smooth, not matted, non-tender, largest 4x5 cm)
B/L axillary LN (mobile, smooth, not matted, non-tender, largest 1x2 cm)
Systems: normal
Pallor+
Multiple B/L cervical & inguinal LN (mobile, smooth, not matted, non-tender, largest 3x3 cm in right inguinal area)
Systems: normal
Ix
Parameters | Values
HB | 13
TLC (DC) | 7.02 (64.3/31.9/0/3.4/0.4)
PC | 61000
ESR | 45 mm/hr
AST/ALT | 685/444
ALP/GGT | 629/265
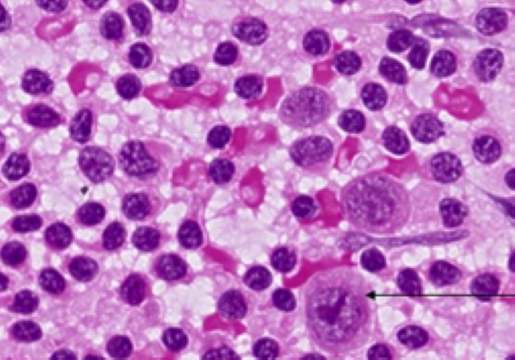
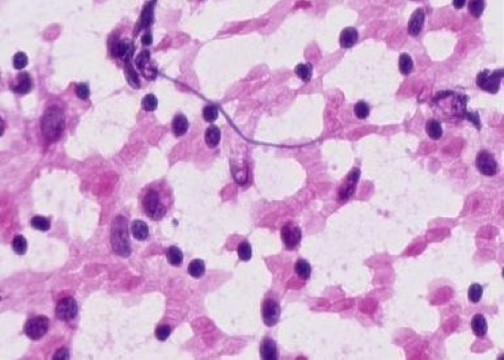
Ab to OX K | 1:80 titres USG neck & axilla: B/L multiple non-matted, cervical and axillary LN with loss of fatty hilum FNAC- (axillary LN) Monomorphic lymphoid cell hyperplasia
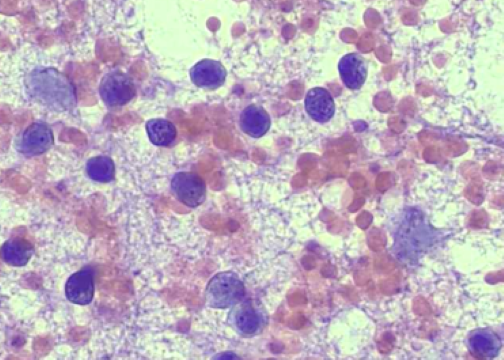
Conclusion: Microbiological/pathological evidence for tuberculosis as mandated cannot be broken. Hence, other differentials also have to be sought even in the presence of constitutional symptoms of tuberculosis and in the absence of laboratory evidence.
Dr Udata Pranavi, Dr Ramya S; Department of Family Medicine, SJMCH
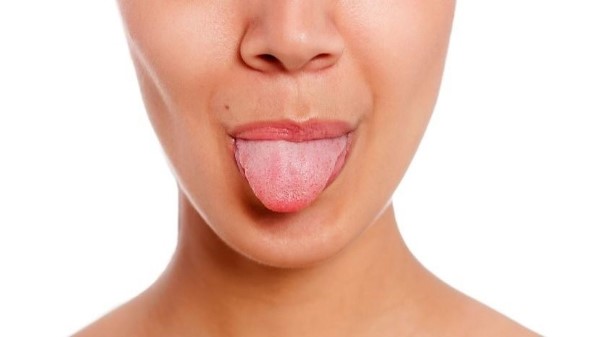
A Silent Side Effect: Ageusia Induced by a Common Diuretic
I wanted to share a recent patient encounter that reminded me to not take any symptom lightly and to always take a thorough drug history.
A 50yr old lady came to me as a patient with some routine health checkup reports. on history taking she began narrating her health concerns over past few months. She had suffered from Bell's Palsy on the left side of the face 3 months back and had been treated by a neurologist for the same and was put on a short course of steroids, multivitamins and lubricant eye drops etc. Over 2-3 weeks, her symptoms improved and she underwent physiotherapy and had regained movement of the face affected by the palsy.
Since then, she had been having altered taste which never improved. In fact, gradually she had completely lost her sense of taste all over the tongue she claimed. This was very distressing for her. She had been attributing it to the Bell's Palsy and was waiting for It to improve but in vain. She had taken some routine health checkup tests before visiting me for a consultation about this loss of taste.
Examination of the oral cavity and rest of physical examination was mostly unremarkable except some residual mild facial asymmetry and her blood parameters were all within normal including thyroid functions, vitamin levels and hemogram.
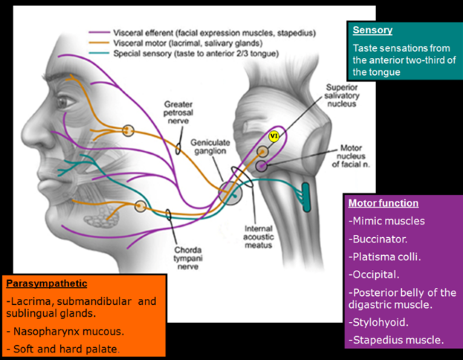
What was puzzling was the loss of taste in all parts of her tongue. In Bell's Palsy, there is loss of taste only in the anterior 2/3rd on the affected side (refer to figure). This is usually compensated by the taste buds in the rest of the tongue and the loss of taste is not very significant.
On further history I found that she was found to be hypertensive as well and around the same time when the Bell's Palsy was diagnosed, she was started on Telmisartan + hydrochlorothiazide combination pill for the same which she had been taking regularly since then.
I then referred her to a neurologist colleague. After a complete evaluation , he felt that the Hydrochlorothiazide could be the possible culprit and suggested we replace with a different drug and observe. Hydrochlorothiazide was replaced with a calcium channel blocker and she was asked to come back for a review after two weeks. And lo and behold, two weeks later she walked in smiling and profusely thankful for getting her sense of taste back.
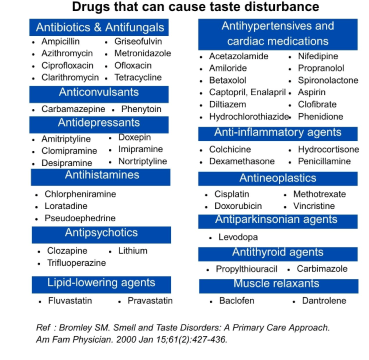
My lesson from this was that even with commonly prescribed drugs we need to be aware of their rare side effects as well. It also prompted me to go and read about other drugs that could affect taste sensation. Sharing the list below.
Fig 6: Drugs affecting taste sensation
Fig 7: Mechanism of taste disorders
Dr Krithika Ganesh
MBBS, DNB (Family Medicine)
Methotrexate in Atopic dermatitis
Mr Shankar, a 76 years old overweight gentleman under my care for chronic asthma, high Blood pressure, also suffers from severe atopic dermatitis. Severe itchy scaly hypertrophied skin all over the body, particularly severe on his legs and arms.
Fig 8: Methotrexate - structure
He was on Dipsalic ointment locally and systemic steroids as and when the atopy became severe. This was the state when he was started on weekly methotrexate, 5mgs once a week with folic acid 5mgs twice a week from February 2021. Dosage gradually upped to 10 mgs once a week which he is presently on now.
There was gradual and excellent response and now except for some acceptable lesions on his feet, the rest of the body has normal skin. For this he uses Methotrexate ointment at bed time.
His liver functions, hemogram, HbA1C have remained normal.
His asthma is under good control with Seroflo 250mcgs twice a day and blood pressure is under control with Seloken 50 mgs and Prazopress 5mgs once a day.
Conclusion
It has been 4 years since this patient is on Methotrexate and the response has been very good. This drug is a good option in severe atopic dermatitis.
B C Rao
Before You Order the Next Test!!
There is a certain silence in clinics these days.
Not the kind that heals. The kind that haunts. A heavy quietness, like something has gone missing. It is the pause before a printer puts out yet another lab report. It is the sound of a patient scrolling through Google beneath the desk, searching for answers they are too afraid to ask out loud.
Fig 9: What to do when blood test results are not quite "normal"
It is the quiet sigh after a rehearsed symptom list, knowing the doctor's already reaching for the prescription pad.
The clock ticks. Not in rhythm with healing, but with the weight of the next patient waiting. And as that white paper tears off with a drug name and a dose, something else deeper goes unheard again.
A pain not captured in tests. A story never told.
A human encounter that could have healed, but did not.
something ancient is being lost here. No, it is not stethoscopes, those are still slung around necks like decorative badges.
What we are losing is Clinical Thinking. The Art of the Pause, The Story, The Timeline, The Uncomfortable Questions.
We are replacing it and dangerously fast with a scroll of investigations.
"Get a CBC, LFT, KFT, TSH, B12, D3, ECG, echo, and HRCT if possible. Just to rule things out."
Rule what out, exactly?
Often, we do not know. But it makes us feel safe. Efficient. Legal. Modern.
But here is a reminder, medicine is not detective work if you test everything before asking the questions. That is just paperwork with a stethoscope!
There used to be a sacred moment in medicine, when a doctor sat down beside the patient and simply listened.
Not clicked. Not scanned. Not interrupted. Just listened.
And in that pause, things would reveal themselves as if the patient's body finally felt heard enough to speak.
For example, let me tell you about Geetha (name changed), 41 years old.
Bank manager. Sharp, punctual, polite.
She came to me after three years of bouncing between doctors and tests.
Her complaint?
Persistent fatigue. Brain fog. Body pain. And "a sense that something is off" severe headaches, fear, and weight loss.
She had done every test you could think of:
Full thyroid panel, ANA panel, Vitamin B12, D3, CRP, ESR, ECG, TMT, 2 MRIs, Hormonal panel
She carried them in a neatly clipped folder. Everything was within range except for a few mild deficiencies, nothing dramatic.
Previous doctors had labelled her:
"Stress-related."
"Fibromyalgia-like."
"Perimenopausal."
"Anxious."
One even started her on neuropsychiatric medications !! which she hesitantly refused to take because it costed her extra money for the strips !
Now here is the part that stayed with me:
She did not cry.
She did not even complain.
She simply said, "I am exhausted, doctor. Not just in the body. In being unheard."
So, I closed her file.
Put away the pen.
And asked, "When did this start?
She thought for a moment. Then looked up and said:
"About three years ago, after my father passed away."
What followed was a full hour of quiet revelation!!! She was the only child. Caregiver for a paralysed parent for six years, returned to work the same day after the funeral. Had not grieved properly. Had many many responsibilities to fill up, many bills to pay, never stopped to catch a free breath, never discussed it with anyone. Husband was quite busy with his work and just sat for dinners and went away, the kids were too small and had to also be looked after by her in every aspect....
She was not sleeping. She had lost all appetite for joy. Her mind was always racing. And yet... she had never once said the word "depression." Because she did not feel "sad" --- just done.
This was not fibromyalgia.
It was not thyroid.
It was not B12.
It was burnout wrapped in duty, silence, and performance.
Her body was not failing. It was protesting. Like a pressure cooker waiting to explode!!
We did not start with a new test.
We started with a pause. Followed by permission.
To rest. To cry. To feel.
To eat like a human again. To stop multitasking. To say no without guilt.
She needed magnesium, protein, and movement, yes.
But more than anything --- she needed someone to believe that her story was enough of a reason to feel unwell.
We are Not Just Over testing. We are Under-Feeling.
Modern medicine is full of progress.
But somewhere, we have become more afraid of uncertainty than of unnecessary testing.
More confident in PET scans than in personal stories.
More trusting on health packages and treadmill tests , ECGs than of body language.
We teach interns to never miss a diagnosis.
But we forget to teach them how to see the person before the pathology.
So, may I suggest bringing back the "Old ...New Rule," Maybe?
Before you order that next test, ask yourself:
Have I heard the full story?
Have I understood the timeline of this suffering?
Did I ask what changed in their life before this began?
Am I ordering this test to help the patient... or to reduce my own discomfort?
Because tests are wonderful.
But they do not replace the moment a patient says:
"No one's ever asked me that before."
And you see the shoulders drop. The room shifts. The story open.
"Do not just test for what is missing in the blood.
Look for what is missing in their life."
A test can guide. But it cannot comfort.
It can diagnose. But it cannot validate pain.
It can confirm a suspicion. But it cannot tell you how long they have been carrying it.
Before you click the next panel,
Try something radical:
Sit back.
Lean in. Ask softly.
And listen like the body is telling you the truth --- because it is...!!
And I bet you
No AI chatbot, scan, or algorithm can replace the healing that happens in a room where one human being truly listens to another.
That is the kind of medicine worth practicing.
Dr Amina Kausar shah
Antiplatelet drugs and anticoagulants
The platelet is fundamental to clot formation especially in the arterial system. Platelet adhesion, aggregation, and activation are the first steps in this process, which is responsible for major catastrophes such as heart attacks, strokes, and acute limb ischemia. Antiplatelet drugs are the sheet-anchor for the prevention and treatment of these life-threatening conditions.
The anti-platelet drugs currently in common use are
Acetyl salicylic acid ( ASA ) - aspirin - 1967
Clopidogrel - 1997
Prasugrel - 2009
Ticagrelor - 2011
Aspirin
The single most widely used drug worldwide. Used as a pain-killer and anti-pyretic since antiquity, its use as an antiplatelet drug began in the late 1960's after John Vane elucidated its effect in inhibiting Prostaglandin production, irreversibly blocking Thromboxane A2 which helps platelets to stick to each other. It is the drug of choice for prevention and treatment of arterial disease in all territories - cardio, cerebro, and peripheral vascular including acute myocardial infarction, chronic coronary artery disease, strokes, Transient ischemic attacks as well as acute and chronic peripheral vascular disease.
Clopidogrel, Prasugrel , & Ticagrelor
The other 3 listed drugs act through a different mechanism. They block a receptor in platelets called the P2Y12 receptor. This blockage prevents platelets from binding to Adenosine Diphosphate ( ADP ) which is a key signal for platelet activation, and setting off the coagulation cascade. Dual antiplatelet therapy ( DAPT ) is mandatory after heart attacks, strokes, coronary and carotid stent implantation, because of the synergistic effect of this combination.
The current combination of choice after coronary stent implantation is Aspirin and Ticagrelor, because it is the most effective in reducing adverse events especially acute stent thrombosis. The disadvantage is a slightly increased bleeding risk. Hence DAPT is used only for 6 -- 12 months after stent implantation. A small subset of patients who do not tolerate Ticagrelor are given a combination of Aspirin and Prasugrel. In other situations where stents have not been used, but DAPT is recommended such as conservatively managed heart attacks and strokes, a combination of aspirin and clopidogrel is preferred as the bleeding risk is less than with the other combinations. Post coronary bypass patient receive single or dual antiplatelet therapy depending on relative risk-benefit assessment.
In the venous system, low flow rates and stasis permits the accumulation of activated clotting factors and local generation of thrombin without a major role for platelets. In the arterial system higher flow rates wash out clotting factors. Therefore, anti-platelet plugs are needed to form a physical barrier and provide a base upon which fibrin clot can form. Deep vein thrombosis and acute pulmonary embolism , as well as clot formation within the atria in atrial fibrillation are classic examples of dangerous often fatal clot formation in the venous system. Antiplatelet drugs have no major role in their prevention or treatment. Instead, anticoagulants need to be used -- parenterally in the acute phase and orally later.
Unfractionated heparin ( UFH )
is in clinical use since 1937. Its advantages are low cost and availability of an antidote -- protamine. Disadvantages are short half-life, less predictable effect, need to monitor and titrate dose and need for IV administration.
Derived from UFH by depolymerization resulting in a smaller, more predictable molecule. Its advantages are longer half-life, more predictable dosing, less need for monitoring, and potentially lower risk of bleeding. Disadvantage is higher cost.
Fondaparinux ( Arixtra )
Synthetic polysaccharide unlike the naturally occurring Heparin, acts very much like LMWH with all its advantages and disadvantage. It has no antidote.
Vitamin K antagonists - Warfarin and Dicoumarol ( Acitrom )
These drugs prevent formation of an active form of Vitamin K which is needed for many clotting factors such as Factors II, VII, IX, and X to participate in the coagulation cascade. Advantages are once daily dosing and low cost. Disadvantages are need for frequent monitoring of lab test, Prothrombin time ( PT ), because of unpredictable effect and need for avoidance of food rich in vitamin K such as cabbage and broccoli. These drugs are mandatory in people with metallic heart valves.
Dabigatran, Rivaroxaban and Apixaban belong to this category, all available for the last decade . This has reduced the usage of vitamin K antagonists because of ease of use, greater efficiency, lack of need for monitoring PT, and greater Time in Therapeutic Range ( TTR ). The only disadvantage is higher cost.
Dr Padmakumar
Iron Over Dopamine? Restless Legs Syndrome Guidelines Revamp
Vincent Richeux
RLS is characterized by an irresistible urge to move the legs, often accompanied by unpleasant sensations such as itching, tingling, or electric paresthesia, which typically affect the lower limbs. It affects 8% of the French population, predominantly women.
New guidelines from the American Academy of Sleep Medicine (AASM) no longer recommend the use of these drugs as first-line treatments.
During the recent French Language Neurology Days in Montpellier, France, Sofiène Chenini, PhD, a researcher at the Sleep-Wake Disorders Unit, Department of Neurology, Gui-de-Chauliac Hospital, reviewed the current treatment approaches for RLS and highlighted non-dopaminergic alternatives. He cautioned that dopaminergic agonists could lead to the augmentation and worsening of symptoms over time.
In France, RLS is guided by the 2019 recommendations of the French Society for Sleep Research and Medicine (SFRMS), which still supports the use of dopaminergic agonists for the most severe cases of RLS.
"For now, we have not updated the guidelines, but we are considering it," said Chenini, referring to the new American recommendations.
Img 10: Restless Leg Syndrome (RLS): Symptoms
Iron as First Line
According to the new AASM guidelines, intravenous iron supplementation is the preferred first-line treatment for severe RLS. In some cases, second-line antiepileptic drugs are considered a first-line treatment option in French recommendations when the severity is low.
These sensations of restlessness typically occur in the evening or at night during periods of rest or inactivity and are temporarily relieved by movement, such as walking and stretching. The condition often leads to repeated leg movements during sleep and difficulty falling asleep due to increased brain activity.
RLS is not fully understood but is often linked to problems with iron regulation.
MRI studies have shown iron deficiency in the brains of patients with RLS. This suggests a disruption in iron transport across the blood-brain barrier and into neurons, possibly due to a decrease in the transferrin receptor.
This disruption in iron regulation, believed to have a primarily genetic origin, induces an increase in the synthesis of dopamine and glutamate, which is likely the cause of the symptoms. In RLS, changes in the dopaminergic system are linked to risk factors such as aging and the use of certain medications.
Five Clinical Criteria
According to a 2016 consensus from the SFRMS, RLS diagnosis is based on five clinical criteria:
An intense and irresistible urge to move the lower limbs accompanied by unpleasant sensations
Worsening symptoms at rest, the patient is unable to stay still
Relief of symptoms through movement such as walking or stretching
Increased severity of symptoms in the evening and at night
The absence of other causes, such as myalgia, fibromyalgia, osteoarthritis, venous insufficiency, and obliterative arteriopathy of the lower limbs
Once diagnosed, iron assessment is required to check for iron deficiency. The analysis includes measuring C-reactive protein to ensure there is no inflammation, "which reduces iron bioavailability," Chenini explained.
Therefore, polysomnography remains optional in such cases. If ferritin levels are below 75 µg/L, iron supplementation is recommended. Treatment also involves addressing factors that worsen symptoms, such as caffeine and alcohol consumption and smoking. It is advisable to stop or switch medications that may aggravate symptoms, such as antidepressants and antihistamines.
The antidepressants involved are serotonergic, particularly serotonin reuptake inhibitors, with a long half-life.
"If stopping treatment is not possible, switching to antidepressants with a short half-life, such as venlafaxine or duloxetine taken in the morning, is recommended," he said.
Lifestyle
For mild RLS cases, lifestyle changes may be sufficient to ease symptoms. These include avoiding coffee, alcohol, and tobacco; maintaining regular sleep and wake times; engaging in physical activity early in the day; and performing stretching exercises before sleeping.
If ferritin levels remain low after 3 months of iron supplementation, switching to intravenous treatment is recommended. Options included a single dose of ferric carboxymaltose (500-1000 mg) or multiple sessions of 200 mg ferric hydroxide-sucrose.
If symptoms persist, a mild opioid is recommended as needed, starting with opium powder, codeine (such as paracetamol-codeine 500/30 mg, up to 60 mg of codeine or more), and tramadol (starting at 50 mg and increasing to 100 mg if necessary).
If the improvement remains insufficient, specific treatment should be considered on the basis of the severity of RLS assessed using the International Restless Legs Syndrome Severity Scale (IRLS) score. Background treatment is recommended for very severe cases (IRLS score above 30), which are linked to the risks for depression and even suicide, as noted by Chenini. It is also advised in cases of severe insomnia or when the quality of life is significantly affected.
A recent study by Chenini and colleagues found a 10-fold higher risk for depressive symptoms in patients with RLS, particularly in young women with insomnia. The study also reported a threefold increase in suicidal thoughts.
Dose and Misuse
According to the French guidelines, very severe cases of RLS require treatment with low-dose dopamine agonists, such as pramipexole, Rotigotine, or ropinirole. These drugs may also help reduce motor inhibition in patients with depression. Dopamine agonists are the only approved treatment for this indication.
"It is essential to respect the maximum dosages," Chenini emphasized. The recommended maximum doses are 3 mg for Rotigotine, 0.54 mg for Pramipexole, and 4 mg for Ropinirole.
Second-line treatments include alpha-2 delta ligand antiepileptics, such as Gabapentin and Pregabalin, especially in cases of severe insomnia. For less severe cases, these antiepileptics are preferred as first-line treatment. Gabapentin may be favored over Pregabalin because it causes less sedation.
The major risk associated with dopamine agonists is worsening symptoms after prolonged use, known as augmentation syndrome, which is particularly higher in patients with iron deficiency, older age, and those prescribed high doses of antagonists.
Concerns about this complication led the AASM to remove dopamine agonists from the recommendations for RLS management.
In 2016, American guidelines similar to the current French recommendations for dopamine agonists were the first-line treatment alongside antiepileptics in the treatment of severe forms of the disease. The new recommendations now place intravenous iron supplementation as the first-line treatment, while antiepileptics are the second line.
Chenini highlighted that this change is due to the misuse of dopamine agonists in RLS. A registry of 670,000 patients with RLS in the United States showed that 60% were treated with dopamine agonists, and 20% received doses exceeding the recommended limits.
The registry shows that neurologists prescribe higher doses of dopamine agonists for RLS than general practitioners. This is likely because these drugs are also used to treat Parkinson's disease, where the doses are approximately 10 times higher than those used for RLS.
Forget the Tremor: These Symptoms Come First in Parkinson's
Markus Vieten
Patients with Parkinson's disease rarely present to the clinic with the textbook signs --- forward stooped posture, slow and rigid movements, or shuffling gait. Instead, the earliest indicators are often vague and nonspecific, though they can later be recognized as early warning signs in retrospect.
By the time the first clear symptoms appear, nearly 50% of dopaminergic neurons are irreversibly lost. The resulting dopamine deficiency disrupts the motor system, leading to hallmark symptoms such as tremor, rigidity, akinesia, and postural instability (TRAP). Diagnosis is clinical, supported by characteristic signs, and often confirmed with imaging (eg, dopamine transporter scan [DaT SCAN]). Onset is usually gradual and progressive, and symptoms may present asymmetrically.
Although Parkinson's disease remains incurable, identifying these early signs before the onset of classic motor symptoms can enable timely monitoring and potential early intervention. The earlier the disease is detected, the better its progression may be slowed. Some symptoms may manifest years in advance.
Below is an overview of early and prodromal Parkinson's symptoms. While most clinicians routinely ask about sleep or gastrointestinal function, the following list may help prompt more targeted follow-up when suspicion arises.
Rapid Eye Movement (REM) Sleep Behavior Disorder (RBD)
Sleep disturbances are often mentioned as early Parkinson's symptoms, but the specific disorder --- REM sleep behavior disorder --- is frequently overlooked. Unlike insomnia or sleep maintenance issues, RBD involves vivid dreaming accompanied by physical movements, such as shouting, punching, or kicking during sleep, often affecting the sleep partner.
RBD occurs in about 0.5%-1% of the population, rising to 5% in those older than 60 years. Importantly, it is considered a prodromal condition for Parkinson's: 80% of those affected may go on to develop the disease within 15 years. Patients reporting these symptoms should be monitored regularly for neurologic changes.
In clinical history-taking, ask specifically about vivid dreams, violent movements during sleep, or vocalizations. Though often dismissed as quirky or anecdotal, recurring incidents should raise red flags.
Constipation
Parkinson's doesn't begin with tremors or slowed movement. Nonmotor symptoms, especially gastrointestinal issues, often appear first. The disease affects the autonomic nervous system, including the enteric nervous system that regulates bowel motility.
There is evidence that pathological changes --- such as alpha-synuclein accumulation --- begin in the gut and olfactory bulb before affecting the brain, aligning with the Braak hypothesis. These protein aggregates can cause constipation or olfactory dysfunction long before motor symptoms emerge.
Studies suggest chronic constipation can precede a Parkinson's diagnosis by 10-20 years. Up to 75% of patients with Parkinson's experience it. While constipation alone is nonspecific, it gains significance when combined with other prodromal signs.
Constipation should raise concern in these contexts:
Persistent, unexplained symptoms.
Co-occurrence with other early signs such as:
Loss of smell (hyposmia).
REM sleep behavior disorder.
Depressed mood.
Fatigue or lack of motivation.
Family history of Parkinson's.
Olfactory Dysfunction
Loss of smell, either partial (hyposmia) or total (anosmia), is another early and often unnoticed sign. Patients may have difficulty detecting even strong odors like coffee, bananas, or pickles.
In Parkinson's, misfolded alpha-synuclein protein aggregates disrupt brain regions, including those responsible for olfaction. These changes may impair neuron function and contribute to early sensory loss.
Animal studies suggest alpha-synuclein may behave like a prion --- spreading through neural pathways. Trials are ongoing to determine whether monoclonal antibodies such as Prasinezumab could help degrade these protein aggregates.
Micrographia
As Parkinson's disrupts dopamine pathways, it impairs fine motor control. Writing --- a highly complex motor task --- often becomes affected. Reduced movement amplitude can lead to smaller, cramped handwriting known as Micrographia.
Micrographia is a typical, though not universal, early motor sign and may precede other motor symptoms. It often appears alongside other signs like a softer, monotone voice or reduced arm swing while walking --- both early signs of extrapyramidal dysfunction.
Classic Motor Signs: TRAP
Parkinson's is commonly associated with:
Tremor: A resting tremor, typically 4-8 Hz, which diminishes with movement (unlike intention tremor).
Rigidity: Muscle stiffness is often described as "cogwheel rigidity" due to a ratcheting resistance during passive limb extension.
Akinesia/bradykinesia: Slowness or poverty of movement, including "freezing" episodes that require verbal cues to initiate or stop movement.
Postural instability: Impaired balance and increased risk of falls, not due to cerebellar, visual, or vestibular dysfunction.
Postural instability is now recognized as a cardinal sign in the TRAP framework. Damage to extrapyramidal reflexes means patients may be unable to catch themselves when off balance.
Additional Early Signs
Depression and anxiety: Often overlooked or misdiagnosed as primary psychiatric conditions.
Reduced facial expression (hypomimia): "Masked" appearance due to reduced facial muscle movement.
Diffuse pain: Especially in the shoulders, back, or arms, sometimes preceding motor signs.
Fatigue: Persistent lack of energy not relieved by rest.
Reduced arm swing: Subtle early sign of movement asymmetry.
When to Refer for Neurological Evaluation
None of these symptoms alone confirm Parkinson's disease, as many are nonspecific or seen in other conditions. However, the presence of multiple early signs --- especially the combination of REM sleep behavior disorder, olfactory loss, constipation, or family history --- should prompt further evaluation.
Referral should ideally be made to a neurologist specializing in movement disorders. A thorough neurologic exam, smell testing, sleep studies (polysomnography), and imaging (eg, DaT SCAN) may be warranted.
Summary Table. Common Early and Prodromal Parkinson's Symptoms
Symptom
Description
Frequency
Lead Time Before Diagnosis
Olfactory dysfunction (hyposmia)
Reduced sense of smell; often the first sign, typically unnoticed
Very common
5-15 years
RBD
Acting out dreams (eg, shouting, punching, or kicking)
Common
10-15 years
Depression, anxiety
Mood disturbance, social withdrawal, loss of interest
Common
5-10 years
Constipation
Reduced bowel motility; often chronic
Common
10-20 years
Pain (shoulders, back, or limbs)
Diffuse musculoskeletal pain
Common
Can occur early
Fatigue
Chronic low energy not improved by sleep
Moderate-common
Years before diagnosis
TRAP
Classic cardinal signs (TRAP), often asymmetric at onset
Very common
Early symptom
Micrographia
Small, cramped handwriting
Common
Early symptom
Hypomimia
Mask-like facial expression
Common
Early symptom
Reduced arm swing
Asymmetry in arm movement while walking
Common
Early symptom
RBD = rapid eye movement sleep behavior disorder; TRAP = tremor, rigidity, akinesia, and postural instability
Identifying these signs early and recognizing meaningful combinations --- not isolated symptoms --- can help clinicians initiate earlier referral and intervention, potentially altering the disease trajectory.
Music Strikes a Chord for Brain Health
Deborah Brauser
June 06, 2025
Music's influence on the brain is documented in conditions ranging from dementia to epilepsy. Both music participation and appreciation are tied to improvements in executive function and memory so how close are we to harnessing music as a targeted therapeutic tool?
One researcher at the forefront of this work is Edward Large, PhD, a professor at the University of Connecticut in Storrs, Connecticut, and director of its Music Dynamics Laboratory. He told Medscape Medical News that he is optimistic about research suggesting that music can help, "not just with depression and anxiety but with more profound neurological and psychological disorders."
However, he added that music's benefits aren't yet fully understood. Robert Zatorre, PhD, founding co-director of the International Laboratory for Brain, Music, and Sound Research in Montreal, Quebec, Canada, cautions against overstating its therapeutic power.
"Music is not a magic pill; it's not a panacea; it doesn't cure everything," said Zatorre who is also a professor at the Montreal Neurological Institute at McGill University, Montreal, Quebec, Canada.
Instead, it's important to define under what circumstances music could be beneficial and in what ways. "And that's where the research is right now" he said.
One challenge is music's deeply personal nature --- what resonates with one person may leave another unmoved. Variables such as culture, age, personal history, social context, and even the nature of the neurological condition can influence how someone will respond to music-based interventions, said Zatorre.
Brain Rhythms and Memory
Large, a former president of the Society for Music Perception and Cognition and a musician himself, believes that one of the most important messages from research is the effect that music has on the rhythm of the brain.
Brain rhythms or waves, also known as neural oscillations, are patterns of brain activity associated with various cognitive processes and behaviors. In healthy brains, slow theta waves (4-8 Hz) and fast gamma waves (30-100 Hz) work together (coupling) to encode and retrieve new memories. Alzheimer's disease (AD) is characterized by disruptions in gamma waves and atypical cross-frequency coupling.
"Music is really the most powerful stimulus we have for synchronizing brain rhythms," said Large.
His group is testing whether stimulating synchrony in the gamma frequency can help treat AD. "That's the frequency at which neurons in the hippocampus synchronize when they're retrieving a memory", he said. Noninvasive, gamma-frequency, auditory-visual stimulation has been shown to improve AD-related biomarkers and memory in animal models.
Large is CEO of Oscillo Biosciences which is developing music based interventions for humans.
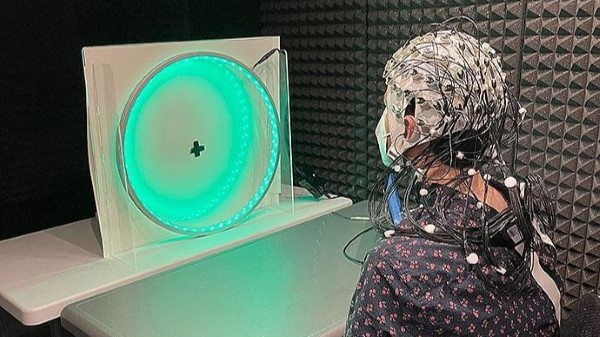
He explained how such interventions might work: The individual listens to self-selected music and watches a rhythmic light stimulus that is synchronized to the music as their brain waves are monitored via electroencephalography. The light show works in concert with the music to stimulate theta and gamma neural rhythms and phase-amplitude coupling (See photo).
It takes both the music and the synchronized light to have a similar effect to that seen for transcranial alternating-current stimulation, he said.
Img 11: An early test of Oscillo Biosciences' music-based intervention for AD
Parkinson's Disease (PD)
In addition to its potential memory boosting, music can help improve motor control.
A music app was shown to improve gait and mood in patients with PD.
Daniel J. Levitin, PhD, a neuroscientist and professor emeritus of psychology at McGill University noted in a recent interview with CBC Radio, that music's steady beat can act as "an external timekeeper" for patients with PD, helping them to walk better because of the auditory stimulation. For multiple sclerosis (MS), Levitin said that music can activate non-demyelinated circuits in order to help with motor control.
He echoed Zatorre's view that while the idea of a music prescription is appealing, what works best for a patient seems to be highly individualized.
"It's not like there is a single healing song or a list of healing songs," he said in the interview. Instead, brain scans show that different types of songs can produce "almost identical" brain activity in the limbic system, which is closely involved in experiencing pleasure, Levitin added.
The Pleasure Principle
The pleasure that music brings may be the source of its positive effects.
Fig 12: Music notes
"I'm convinced that a lot of the benefits of these musical interventions act via the reward system," said Zatorre who has conducted several related studies and authored a chapter on "Musical Enjoyment and the Reward Circuits of the Brain" for a book on Music and Mind edited by opera singer Renée Fleming.
By engaging the reward system "it has knock-on effects on a lot of behaviors and cognitions, including social cognition and memory and language," he said.
Zatorre theorized that music heard by a patient with a memory disorder will activate the reward pathway and simultaneously enhance the retrieval of certain memories. "That's something that has been observed anecdotally in many patients with neurodegenerative disorders," he said.
There is evidence that the connectivity of the auditory and reward systems is preserved in people with mild cognitive impairment and early AD opening up a potential pathway for early treatment. "I'm not sure we're there yet. But it's something that people are excited about," said Zatorre.
Familiar music tends to elicit a greater neural response, especially in older people, because once we reach a certain age, we know what we like and sticking to that brings enjoyment, which is linked to dopamine, explained Zatorre.
The reward system is highly reactive in younger people. "We not only fall in love with people [more easily] at that age, we fall in love with all sorts of things and places and movies and music. And that tends to stay with us," Zatorre said.
Large is currently conducting a functional MRI study in patients with AD that compares music that is self-selected and "meaningful" to the participants with music that is merely familiar.
The meaningful music activates important parts of the brain such as the auditory cortex, hippocampus, and reward centers more than the familiar music, he reported. "So if you're trying to have an impact on your brain, I think you should listen to the music that you love."
Sing Like There's Nobody Listening?
A number of recent studies have suggested that physically participating in music may be even better for the brain than passively listening (Figure).
Fig 13: A person playing keyboard
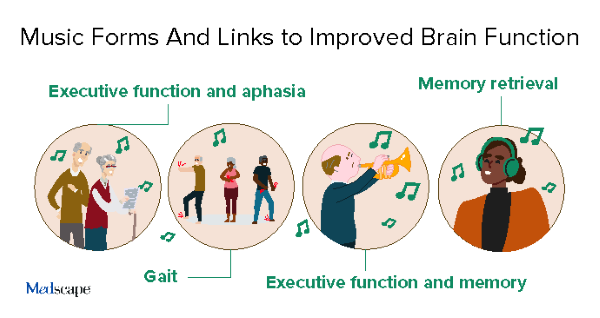
In a large nested study published last year, playing a musical instrument was linked to better executive function in older adults, with stronger links for woodwind instruments.
Keyboard playing was associated with better working memory compared to not playing any instrument. This study did not show any significant associations between listening to music and cognitive performance but singing was associated with better executive function.
Img 14 - Music Forms and Links to Improved Brain Function
Group singing may be particularly beneficial. A Finnish study tied singing in a choir to enhanced brain-structure connectivity across the lifespan of participants with no neurologic diagnoses at baseline.
Another recent study in 50 patients with chronic aphasia after stroke found that those assigned to participate in weekly sessions of group singing had improved communication and responsive speech production 5 months later compared to those who received standard of care.
"It has to do with the vocal motor control, the ability to control your larynx and your breathing and your articulators, as well as the vocalization that singing requires as opposed to speaking," said Zatorre, who was not involved with the research.
He added that the social aspect of the intervention is also important, especially the "singing together with other people who are suffering the same difficulties as you."
But what about people with congenital amusia ie, the tone deaf? Zatorre noted that about 50% of people who are tone deaf have perfect rhythm. "They may not have the pitch correct, but they still are on time. So they can clap, or tap, or march, or dance, along to the beat," he said.
While many may think they are tone deaf, it's estimated that only 1.5%of the general population have true congenital amusia and even fewer also have no rhythm. "They may not enjoy the music itself but could enjoy the more social aspects of it. It's enjoying bonding with others, even if you're singing off-key," said Zatorre.
He pointed out that patients with aphasia usually don't sing very well, "but that's not the point." Instead, the goal is improved outcome, he added. As the saying goes "sing like there's nobody listening."
Music As Preventive Medicine?
Could music be used as a preventive intervention to stave off, say, dementia in younger at-risk individuals?
"I think the answer is [that] we don't really know," Large said. Although there are still questions about whether amyloid beta (Aβ) plaques are a cause or a symptom of AD, it's been shown that there is a desynchrony of rhythms in the gamma frequency band before a buildup of Aβ plaques occurs, he explained.
"I think that offers some hope that these rhythm-based therapies might have a preventive impact," said Large.
Zatorre acknowledged that research on music as a preventive intervention is "quite scarce," but noted that adding music can still improve quality of life.
"Music is an important art form that almost all people are sensitive to. If you're having a better quality of life, that will enhance everything. Even if it doesn't prevent the formation of plaques in your brain, you will still have a happier existence. And then if you do develop any type of degenerative disorder, you'll have more tools in your toolbox to help you cope," he said.
However, Zatorre noted that the same could be said for cooking or exercise or anything else that gives pleasure to an individual.
"I worry that music may have been a bit oversold to people, especially from those who are promoting a website or some type of self-help product. So I think caution is in order," he said.