Table of Contents
Messages

Message from the National President, AFPI – Dr. Mohan Kubendra
Dear Colleagues,
It gives me great pleasure to write this message for the AFPI Karnataka State Chapter Newsletter. As the founding president of this vibrant chapter, I feel a deep sense of pride and joy in witnessing how far we have come together in our collective journey to strengthen and promote Family Medicine.
Over the past year, the Karnataka Chapter has made outstanding contributions at both the state and national levels. Hosting the WONCA South Asia Regional Conference 2025 in Bengaluru is a landmark achievement that reflects the chapter's leadership, organizational strength, and commitment to the discipline. Beyond this, the chapter has continued to excel in academic engagement, organizing impactful CMEs, workshops, and training programs that have benefited practitioners, residents, and medical students alike. These initiatives have kept the spirit of Family Medicine alive, vibrant, and evolving. I sincerely thank the leadership team and all members of AFPI Karnataka for their tireless efforts and vision in promoting our specialty across various levels of healthcare and education.
As we reflect on the broader landscape, it is evident that Family Medicine today stands at a defining moment in India's healthcare evolution. For centuries, family doctors have been the trusted custodians of community health-addressing not just diseases, but the person as a whole, in their social and familial context. The rapid rise of specialization and corporatization have, however, distanced healthcare from its community roots. As healthcare shifts from selective to comprehensive primary care, incorporating wellness, mental health, and continuity of care, Family Medicine specialists are best placed to meet these emerging needs.
At the same time, we are entering an era shaped by Artificial Intelligence (AI) and digital transformation. While AI will undoubtedly revolutionize diagnostics and data interpretation, it cannot replace the human connection, empathy, and trust that define our profession. Family Physicians will continue to serve as the bridge between technology and humanity-interpreting information, contextualizing care, and supporting patients through compassion and continuity.
Family Medicine is more than just a medical specialty—it is a philosophy of care. We are the first point of contact for individuals and families, walking WITH them through every stage of life. To my younger colleagues and medical students: the future of healthcare rests in your hands. I encourage you to see Family Medicine not just as a career option, but as a calling to serve society in its truest sense. Each patient you care for, each family you support, and each community you uplift brings meaning to your journey.
AFPI remains steadfast in its mission to advocate for structural reforms in medical education and health policy that will enable the growth of Family Medicine as the cornerstone of India's health system. Together, with Karnataka leading by example, we will continue to ensure that every individual and family has access to competent, compassionate, and comprehensive care close to where they live.
Heartiest congratulations to the editorial team of the Newsletter.
With warm regards and best wishes,

Message from the State President, AFPI – Dr. Sowmya B. Ramesh
Greetings to all my dear colleagues across Karnataka and beyond.
It gives me great pleasure and honour to share that we successfully conducted our State Conference at St. John's under the theme "At Every Age and Every Stage – Family Medicine for Women and Child Care."
The conference was attended by over 240 delegates from across Karnataka, including Belagavi, Mysuru, Tumakuru, Bidar, and also from neighbouring states such as Kerala, Tamil Nadu, Andhra Pradesh, Maharashtra etc. We were privileged to have Padmasri Dr. C. N. Manjunath sir as our Chief Guest. With the active participation of health visionaries and policy makers, this event truly took Family Medicine to new heights.
Alongside the conference, we also conducted a Dementia Training Program, which was attended by over 80 delegates. The participants received online training on the basics of dementia, including diagnosis and assessment tools.
Looking ahead, we have more academic activities planned. In the first week of December, we will be hosting a hands-on Dysphagia Workshop. Additionally, a webinar on health management is in the pipeline.
We sincerely hope that the coming year will bring us many more insightful and practically useful sessions. I warmly invite all of you to share your thoughts, suggestions, and ideas to make our initiatives even more meaningful.

From the Secretary's Desk – Dr. Hemavathi D
Reflections on the 5th AFPI Karnataka State Conference
It gives me great pleasure to share my reflections on the recently concluded 5th AFPI Karnataka State Conference. Serving as the Scientific Chair for this landmark event was both an honour and a deeply enriching experience.
The conference brought together a vibrant community of family physicians, residents, and medical educators from across the state and beyond, united by the shared goal of advancing the practice.
Our theme — "Every Stage, Every Age: Family Medicine transforming Women and Child" guided the scientific program, ensuring that every session resonated with the current challenges and aspirations of primary care practice.
The scientific committee aimed to design a program that was comprehensive, relevant, and engaging, balancing academic rigour with practical applicability.
The agenda included plenary sessions, panel discussions, skill-building workshops, oral and poster presentations and interactive case discussions.
Topics ranged from medical conditions during pregnancy, recent advances in labour, Immunization, adolescent care, child adoption and ovum preservation to innovations in digital health and primary care research.
The conference witnessed enthusiastic participation from over 180 delegates, including family physicians, postgraduate students, and young practitioners. The active academic engagement of residents through research presentations (40 posters and 20 oral presentation) was a heartening sign of scholarly interest in Family Medicine.
Feedback from participants has been overwhelmingly positive, highlighting the relevance of topics, quality of speakers, and the opportunity to interact and network with peers and mentors. Many expressed that the sessions have inspired them to integrate newer perspectives into clinical practice and explore research avenues within their communities.
Organizing the scientific program was a journey of learning, teamwork, and shared commitment. It was deeply rewarding to see the enthusiasm and energy that permeated every session, reaffirming the strength and unity of our fraternity.
I take this opportunity to express my sincere gratitude to the organizing committee, session chairs, faculty, volunteers, and all participants who contributed to making the 5th AFPI Karnataka State Conference a grand success. Together, we continue to uphold the vision of AFPI – to strengthen Family Medicine as the foundation of comprehensive, continuous, and compassionate healthcare for all.
Editorial Notes

Journey of Dr. B.C. Rao – The Editor
10 years with a small intermission, is a fairly long term to hold any office, much less that of editorship of a newsletter cum journal.
I am happy that my repeated requests to be relieved have at last found receptive ears and my young friend Amina Shah, has taken over and the October issue onwards it will be her effort.
The newsletter should serve two purposes. One is to provide information as to the activities of both the central and state bodies of AFPI. The other is to act as a medium to give exposure to professional talent. Many case reports, articles, experiences go unpublished due to lack of a medium and the difficulties that one must go through to get published in national peer reviewed journals. Our AFPI newsletter has tried to bridge the gap.
What it has failed to do is to reach out to young doctors and trainees and trainers on a bigger scale. Here is where I have failed and I wish Dr Amina Shah will succeed given her age and enthusiasm.
I wish her all the best.
A New Chapter Begins – Dr. Amina Kausar Shah
As I take over the mantle of Editor of the AFPI Karnataka Newsletter, I do so with a deep sense of gratitude and responsibility. For nearly a decade, Dr. B. C. Rao has nurtured this publication with dedication, wisdom, and quiet perseverance. His vision transformed it into more than a newsletter — it became a chronicle of our collective journey as family physicians. I am deeply thankful for his guidance and for trusting me to continue what he so gracefully built.
In today's rapidly evolving landscape, our newsletter must not only inform but also inspire. My vision is to make it a vibrant, interactive platform — a space where ideas, innovations, and experiences of family physicians, young doctors, and trainees can find voice and visibility. We aim to blend science and stories, evidence and empathy, so that each edition reflects both our profession's rigor and its heart.
As we turn this new page, I invite every member — senior or student — to write, share, question, and contribute. This is your space. Let's make it one that sparks conversation, connection, and change.
Scientific Sessions Update – October 2025

The past few months have been eventful and enriching for AFPI Karnataka, marked by active academic engagement and collaborative learning.
July 19th–20th: The 7th Practical Exam Orientation Session was conducted at Bangalore Baptist Hospital, helping postgraduate students gain hands-on insights and confidence for their upcoming practical examinations.
August 2nd–3rd: The 5th State Conference was successfully held, focusing on "Women and Child Health." With an attendance of nearly 200 delegates, the event brought together enthusiastic PG students and experienced family physicians. The conference was graced by Dr. C. N. Manjunath as Chief Guest, and hosted with generous support from St. John's Medical College. It was indeed an academic treat for all participants.
Beyond these academic activities, AFPI Karnataka continued its tradition of community and professional collaboration:
- Extended support to NGOs, encouraging family physicians to participate in the treatment of rare diseases.
- Supported AFPI Telangana and Andhra Pradesh State Conference on August 30th–31st through active participation.
- Continued the "Back to Benches" monthly certificate course for practicing doctors, organized in collaboration with FFPAI.
- Partnered with the Dementia India Alliance to mark World Alzheimer's Month by organizing an online certificate course on Dementia Basics (September 18th–19th), which saw participation from family physicians across India.
In addition, our members continue to contribute individually to academia and public health through their independent programs on GLPs, Sarcopenia, Policy Making, and several other topics. Many have also organized health camps, vaccination drives, and community outreach activities.
With such enthusiastic involvement from every member, Family Medicine in Karnataka continues to grow, inspire, and thrive.
Events & Highlights
AFPI KARNATAKA 5TH STATE CONFERENCE 2025
"At every stage, At every age: Family medicine transforming women and child health"
2nd & 3rd August 2025, Bengaluru
Venue: St Johns Medical College, Bengaluru, Lecture Hall 1, Golden Jubilee Block
The Big One - AFPI Karnataka 5th State Conference 2025





200 delegates | 3 workshops | 4 panels | 11 paper presentations | 1 theme – Women & Child Health
Venue: St. John's Medical College, Bengaluru
Dates: August 2nd–3rd, 2025
The 5th State Conference of AFPI Karnataka, held at St. John's Medical College, Bengaluru, was a vibrant confluence of knowledge, skill, and camaraderie.
With the theme "Women and Child Health," the event brought together over 200 delegates — postgraduate students, young practitioners, and senior family physicians — for two days of hands-on learning and meaningful dialogue.
The conference was inaugurated by Dr. C. N. Manjunath, who highlighted the indispensable role of family physicians in preventive and community-based care. The inaugural address set the tone for an event rich in academic rigor and practical relevance.
Hands-On Workshops
The pre-conference workshops held in collaboration with St. John's Department of Family Medicine were a huge draw. Sessions on clinical examination and procedural skills, point-of-care ultrasound, and emergency medicine for primary care allowed participants to refine essential clinical competencies under expert guidance.
Scientific Sessions
The scientific sessions that followed were dynamic and thought-provoking.
A debate on GLP-1 agonists explored both promise and pitfalls in diabetes management. The panel on cord blood and ovum preservation opened fresh perspectives on the role of family physicians in reproductive health.
Another highlight, "From Bench to Bedside: Translating Gut Microbiome Discoveries into Practice," brought research to relevance for day-to-day clinical decision-making.
Post-lunch discussions explored sensitive yet timely themes such as adoption and the GP's role in supporting families beyond biology, reflecting AFPI's broad, humanistic approach to medicine.
Research and Poster Presentations
The conference also celebrated academic excellence through oral and poster presentations by postgraduate students. Topics ranged from family medicine reforms, diabetes care, and lifestyle interventions to rare diseases and community-based challenges, showcasing the intellectual depth and diversity of upcoming family physicians.
The event concluded with a valedictory ceremony and prize distribution, acknowledging the best research papers and posters. The conference stood as a testimony to AFPI Karnataka's mission — to make family medicine the cornerstone of holistic, evidence-based healthcare.
Rural Karnataka – Bustling Energy

Karnataka Brain Health Initiative – Vijayapura
Arjunagi Village Camp: Reaching the Unreached
The Karnataka Brain Health Initiative (KaBHI) – Vijayapura, under the Department of Geriatrics at Shri B.M. Patil Medical College and Hospital, organized a rural outreach camp at Arjunagi village, Babaleshwar Taluk, on January 26, 2025, as part of the "Reaching the Unreached" program. The camp focused on promoting brain health, dementia screening, and fall-risk assessment among the elderly.
Highlights of the Camp
- Participants: elderly individuals (aged 60+)
- Team: Physicians, Psychologists, Physiotherapists, and Unani interns from KaBHI
Activities Conducted
Neurology and Dementia Awareness: Dr. Yasin (District Coordinator) and team conducted sessions addressing myths about neurological disorders—especially epilepsy—and emphasized early medical intervention and the goals of the KABHI program.
Dementia Screening: Dr. Bharath Sarguru led cognitive screening using the HMSE tool, assessing 34 participants. Findings: 33 participants scored above 18, while 1 showed cognitive decline, highlighting the value of early detection.
Fall-Risk Assessment: Physiotherapist A.M. Likitha performed fall-risk evaluations. Among 10 assessed, 4 had Berg Balance Scores below 45, indicating fall risk. Strengthening, balance, and coordination exercises were demonstrated to patients and caregivers.
Training & Capacity Building
Unani interns gained hands-on experience in dementia screening and geriatric care, strengthening interprofessional learning. They emphasized that this outreach helped them appreciate early diagnosis, teamwork, and community engagement.
Outcome
The camp successfully improved awareness of neurological health, trained healthcare interns, and empowered the elderly to adopt preventive practices for healthy aging.
The KABHI team plans to continue such monthly rural outreach programs to ensure brain health for all.
Academic Columns


The Dr. B.C. Rao Column – Pearls of Wisdom
Practice Experience – A Small Beginning, A Big Impact
Often in one's professional life, a small clinical decision can lead to a major outcome.
The following true story is one such reminder.
About ten years ago, Mrs. Rajani Seroo consulted me for a minor ailment. Her initial investigations revealed a high ESR without an obvious cause, along with a borderline increase in the globulin fraction on liver function testing. Ordinarily, this might have been dismissed as insignificant. However, the persistently high ESR caught my attention.
On a hunch — more than any diagnostic brilliance — I ordered a serum protein electrophoresis, which revealed a prominent single gamma spike, suggestive of Monoclonal Gammopathy of Uncertain Significance (MGUS). This explained her elevated ESR.
MGUS can remain silent and stable for years, but in some cases, it progresses to plasma cell disorders such as multiple myeloma, Waldenström's macroglobulinemia, or certain types of lymphoma.
Further evaluation in Mumbai confirmed that Mrs. Seroo had Waldenström's macroglobulinemia.
Here's where the story takes an inspiring turn and the interesting part — Rajani realized that there was no support group or organization for people living with MGUS or Waldenström's in India. Motivated by her own journey, she and her son Saurabh Seroo founded Waldenström India in 2019 (www.wmindia.org). To guide these sufferers as to how to manage, where to seek help, and in short, a support system was badly needed.
Since then, they have supported and guided numerous patients, creating a much-needed platform of hope and awareness.
Sometimes, what begins as a small clinical curiosity can blossom into a movement that transforms lives.
The Family Medicine Frontiers: Dr. Madhavi – Pioneering in Palliative Medicine
What Is Palliative Medicine?
Palliative medicine is a comprehensive, patient-centered approach to treating people with life-limiting illnesses, whether they are cancerous or not. Its goal is to minimize suffering and improve quality of life. Contrary to popular belief, palliative care is not just for people who are nearing the end of their lives; it includes much more. It might begin at any point in the disease's progression as in Regardless of the prognosis, it manages medical symptoms, psychological and spiritual problems, and caregiver support, thereby improving curative or life-extending therapies.
Why Is It Crucial in Family Medicine?
Family physicians are uniquely positioned to champion palliative care in the community. Our relationship with patients and families—often spanning years or even generations—gives us unparalleled insight into their values, cultural contexts, and health journeys.
Role of Family Physician
- Recognizing when a patient may benefit from early palliative support.
- Having open, empathetic conversations about goals of care and patient preferences.
- Managing common symptoms effectively.
- Supporting families and caregivers, who are often under equal stress.
In practice, palliative medicine is about shifting focus from "just adding years to life" to "adding life to years." Family physicians, with their long-term relationships with patients , are uniquely placed to introduce and normalize palliative care, ensuring dignity, comfort, and support in patients' lives.
With the growing number of people living with serious or chronic illnesses, it's more important than ever to make palliative care a routine part of family practice. When family doctors are equipped with the right training, they can provide timely and compassionate care. Integrating palliative care into everyday medical practice ensures patients don't just live longer—they live well.
Era of the Smart AI Doctor – Dr. Syed Mubarak
AI in Medicine: Transforming Healthcare
In today's rapidly changing world of medicine, technology isn't just assisting doctors — it's transforming the very way we practice. From diagnosis to decision-making, the modern physician must evolve into a Doctor 2.0 — one who understands, embraces, and ethically applies Artificial Intelligence in patient care.
Artificial Intelligence (AI) is a powerful technology that enables machines to perform tasks normally requiring human intelligence. It involves computers learning from large amounts of data to understand, reason, and generate human-like responses. In simple words, AI can "think" and learn from experience to help solve problems faster and more accurately.
AI is reshaping the medical field by improving diagnosis, personalizing treatment, assisting doctors and nurses, and making healthcare more accessible especially in countries like India with limited resources. AI can analyse medical records, scan images like X-rays or MRIs, predict diseases early, and automate routine tasks —making healthcare efficient and reducing human errors.
AI in the medical field in India has huge potential, both for everyday patient care and in hospitals.
Outpatient Department (General Physician)
- AI can help doctors diagnose illnesses faster and more accurately using smart assistants that analyse symptoms, medical history, or lab reports.
- Virtual health assistants (like chatbots) can answer common health questions, book appointments, send reminders, and guide patients about dos and don'ts before or after a visit.
- AI can also read and interpret scans such as X-rays or ECGs, highlight urgent issues, and suggest possible next steps to the doctor—making it easier to manage more patients with less time.
- In areas lacking specialists, AI helps GPs refer patients to the right expert or identify high-risk cases for follow-up.
In-Patient Care (Hospital Setup)
- AI systems track patient vitals, alert staff to sudden changes, and help in preventing critical emergencies by detecting problems early—even at night or when staff is busy.
- For hospitalized patients, AI can manage medicine dosages, schedule investigations, predict who might need ICU care, and help doctors make better treatment choices by analysing large amounts of medical data.
- AI-driven robots assist in surgeries, reduce human errors, and support repetitive but important tasks like monitoring fluid intake or reminding about physiotherapy sessions.
- AI can also help hospital management optimize bed allocations, track patient flow, and even predict disease outbreaks within the facility.
Popular Large Language Models (LLMs) and Their Best Uses
LLMs are AI models that understand and generate human language, helping doctors and healthcare providers in many ways. Some common LLMs and their best uses include:
- GPT-5 (OpenAI): Great for complex clinical decision support, generating medical reports, and coding assistance.
- Claude Opus 4 (Anthropic): Excels in drafting detailed research summaries and assisting with evidence-based writing.
- Gemini 2.5 Pro (Google): Known for integrating text with images and other data to support diagnostics.
- Grok 4 (xAI): Useful for real-time web information retrieval and patient data analysis.
- Llama 4 Scout (Meta): Popular among developers for customizing AI assistants in healthcare apps.
LLMs Used in India's Medical Field
- Med-PaLM 2 (Google): Clinical reasoning and answering medical questions.
- OpenBioLLM-70B (Saama): Biomedical research and genomics analysis.
- BioGPT (Microsoft): Drug discovery and biomedical text generation.
- BioMedLM (Stanford): Biomedical literature mining and clinical NLP.
- August AI (India-based): Focused on regional language support and patient education.
Current Real Examples of AI in Medicine
- IBM Watson for Oncology: Helps oncologists create personalized cancer treatment plans by analysing clinical data and medical literature.
- IDx-DR: An AI system used in India and globally to screen diabetic retinopathy from retinal images, enabling early detection of this vision-threatening condition.
- DeepMind's Kidney Injury Predictor: Predicts acute kidney injury hours before it happens, allowing timely treatment to reduce risks.
- AI-powered Radiology Tools: Used in many hospitals in India for interpreting X-rays and CT scans rapidly.
- AI Chatbots in Telemedicine: Startups in India use LLM-powered chatbots for multilingual patient interaction, appointment scheduling, and medical advice, improving rural healthcare access.
- Diagnostic Labs in India: Some labs use LLMs to auto-generate diagnostic summaries from pathology reports, reducing manual effort and improving report quality.
Future of AI in Medicine: Growing Areas
- AI-Driven Personalized Medicine: Tailoring treatment based on genetics, lifestyle, and medical history.
- Robotic-Assisted Surgery: Increasing precision and reducing errors in complex surgeries.
- Predictive Analytics for Preventative Care: AI predicting disease risks and outbreaks for timely interventions.
- Virtual Health Assistants: Providing continuous remote patient monitoring and managing chronic disease care.
- AI in Drug Discovery: Accelerating the development of new drugs through simulation and analysis of biological data.
AI holds tremendous promise for revolutionizing healthcare in India and worldwide. It empowers doctors and nurses with better tools, enables faster, more accurate diagnoses, and bridges gaps in healthcare accessibility. By adopting AI-powered solutions, the medical field can offer personalized, efficient, and high-quality care to millions.
As AI continues to evolve, its thoughtful integration into healthcare will lead to improved patient outcomes.
This article invites medical professionals to embrace and explore AI as a partner in their daily practice—one that amplifies their expertise and frees them to focus more on compassionate care.
Clinician's Desk
Young guns fire!! Bringing the best of all the Posters Presentations - The Young and Brilliant Generation
A Limping Clue: Viral Myositis with Alarming CPK
Introduction
Viral myositis is a common paediatric condition following influenza A & B virus infections. Although usually self-limiting, severe forms can cause muscle weakness, rhabdomyolysis, and life-threatening complications. Recognizing non-respiratory manifestations of influenza helps avoid morbidity and mortality.
Objective
To emphasize the importance of considering viral myositis as a differential diagnosis in children presenting with acute limb weakness following a viral illness.
CASE 1: 7-YEAR-OLD GIRL
Presentation:
- Fever 7 days prior
- Severe leg pain for 5 days
- Progressive limping to inability to walk
- Lower limb power: 2/5
- Stiffness and restricted movement
Key Investigations:
| Parameter | Result |
|---|---|
| CPK | >10,000 |
| Urine protein/creatinine ratio | 14.7 |
| R6 Bio fire | Influenza B positive |
| Dengue, Leptospira | Negative |
| MRI | Dermatomyositis pattern |
| Muscle biopsy | Necrotizing myopathy |
Hospital Course:
Lower limb Doppler ruled out DVT. Managed with oseltamivir, hydration, and analgesics. Developed rhabdomyolysis and AKI; responded well to IV fluids and steroids. CPK levels reduced, and the child was discharged in a stable state.
CASE 2: 6-YEAR-OLD GIRL
Presentation:
- 4-day history of fever, headache, and dry cough
- Thrombocytopenia (55,000)
- Limping with severe lower limb pain
- Bilateral lower limb power: 3/5
Key Investigations:
| Parameter | Result |
|---|---|
| CPK Levels | 6410 → 2310 → 1007 |
| SGOT | 1720 |
| Serum Creatinine | 0.4 |
| Na/K | 129/5.18 |
| R6 Bio fire | Influenza A-H3 |
Management:
Oseltamivir, IV fluids, and analgesics. Discharged stable with normalizing CPK.
Differential Diagnosis
- Benign Acute Childhood Myositis (BACM)
- Myalgia associated with viral infection
- Dermatomyositis
- Guillain-Barré syndrome
- Muscular dystrophy
- Hypokalaemia
- Poliomyelitis
Conclusion
Family physicians are often the first point of contact for children with flu-like illness. Awareness of non-respiratory complications such as viral myositis enables early diagnosis, supportive management, and prevention of severe complications including renal failure, arrhythmias, and respiratory distress.
References
- Hyczko AV, Rohrbaugh MK, Suliman AK, Hackman NM. A crawling case of benign acute childhood myositis. SAGE Open Med Case Rep. 2021 Sep 17;9:2050313X211047321. doi:10.1177/2050313X211047321.
- Chen HW, Chang MC, Wang TL, et al. Benign acute childhood myositis in the COVID-19 era: how does it compare to influenza? Eur J Pediatr. 2025;184:291. doi:10.1007/s00431-025-06116-6.
Clinical Audit Highlight
A Clinical Audit on Drug Adherence Among Patients Attending OPD, IPD, and ICU
INTRODUCTION
Poor medication adherence remains a major barrier to achieving optimal treatment outcomes in chronic diseases. It contributes to disease progression, increased hospitalizations, and higher healthcare costs. This audit aimed to evaluate adherence patterns and identify factors contributing to non-adherence among patients attending OPD, IPD, and ICU.
OBJECTIVE
- Assess the prevalence of medication adherence among patients.
- Identify factors contributing to non-adherence and recommend strategies for improvement.
- Study complications associated with non-adherence and compare them with those in adherent patients.
METHODOLOGY
- Study Population: Patients attending OPD, IPD, and ICU.
RESULTS
Reasons for Non-Adherence (n=16)
| Reason | Percentage |
|---|---|
| Forgot to take medication | 81.3% |
| Experienced side effects | 12.5% |
| Felt better and stopped taking | 25% |
| Did not understand importance | 37.5% |
| Medication too expensive | 6.3% |
| No family support | 18.8% |
| Fear of dependency | 6.3% |
| Ran out of medication | 25% |
DISCUSSION
Low adherence (45.2%) is concerning, especially in chronic illnesses like diabetes and hypertension. Contributing factors include lack of awareness (59.5%), lack of family support (74.4%), and frequent forgetfulness (81.3%). Only 3 out of 13 patients (23.1%) met optimal adherence criteria.
Medication non-adherence leads to suboptimal disease control, increased hospital readmissions, and higher healthcare costs. Education, reminder systems (pill boxes, alarms), and family involvement are vital interventions.
SUGGESTIONS FOR IMPROVEMENT
- Reinforce patient counselling at every OPD visit.
- Provide printed instructions in local language.
- Encourage use of reminder aids (pill boxes, alarms).
- Engage family/caregivers in follow-up planning.
- Implement telehealth-based medication tracking systems.
CONCLUSION
Medication adherence is a critical determinant of clinical outcomes. Interventions focusing on patient education, simplified drug regimens, and enhanced communication between physicians and patients can improve adherence and reduce long-term complications.
REFERENCES
- Medication adherence influencing factors—an updated overview of systematic reviews.
- Zimring M. Medication adherence among persons with cardiovascular diseases. 2024.
- Jaideep C. Menon et al. Empowering patients for better adherence. AFPI Karnataka 2025.
The Update Dose
Latest Update: 2025 ACC/AHA Hypertension Guidelines – A Shift Toward Early and Holistic Control
The American College of Cardiology (ACC) and American Heart Association (AHA) have jointly released the 2025 High Blood Pressure (Hypertension) Guideline on August 14, 2025, replacing the 2017 version. This major update reflects an evolving understanding of cardiovascular and cerebrovascular risk and places greater emphasis on prevention, personalized care, and adherence.
1. The New PREVENT Risk Equation
One of the most notable changes is the adoption of the PREVENT risk equations to guide treatment decisions, replacing the older Pooled Cohort Equation. The PREVENT model integrates modern population data and offers more accurate predictions of 10-year and lifetime cardiovascular risk, accounting for broader risk factors such as social determinants of health. This change allows clinicians to better identify patients who would benefit from early pharmacologic intervention, especially among younger adults and women.
2. Refined Approach to the "Elevated" BP Range
The 2025 guideline adopts a more proactive approach to treating individuals with systolic BP between 130–139 mmHg or diastolic BP between 80–89 mmHg. After 3–6 months of lifestyle modification, if blood pressure remains above goal, medications may be initiated—particularly if the patient's PREVENT score shows elevated cardiovascular risk. This marks a shift from "wait and watch" toward early, targeted intervention to prevent long-term organ damage.
3. Focus on Subgroups
Specific recommendations are now outlined for chronic kidney disease (CKD), pregnancy, and resistant hypertension:
- In CKD, ACE inhibitors or ARBs remain the preferred initial therapy, with closer monitoring of renal function and potassium levels.
- In pregnancy, methyldopa and labetalol continue to be preferred, while the guideline strongly discourages ACE inhibitors, ARBs, and renin inhibitors.
- Resistant hypertension management now includes guidance on combining mineralocorticoid receptor antagonists with other drug classes and assessing secondary causes more systematically.
4. Emphasis on Team-Based and Home-Based Care
Recognizing that adherence remains a key barrier to control, the 2025 guideline advocates a team-based approach—involving physicians, nurses, pharmacists, and health coaches—to optimize follow-up and support. Home blood pressure monitoring (HBPM) and telemedicine are strongly encouraged as tools for both diagnosis confirmation and ongoing control.
In addition, the guideline recommends single-pill combination therapy as the preferred first-line approach for most patients, improving adherence and reducing pill burden.
5. Hypertension and Brain Health
A major highlight of the new document is the explicit linkage between blood pressure control and cognitive outcomes. The guideline underscores strong evidence that maintaining optimal BP reduces the risk of dementia and cognitive decline, positioning hypertension control as a cornerstone of healthy brain aging.
In Summary
The 2025 ACC/AHA Hypertension Guideline signals a paradigm shift—from reactive management to proactive prevention. With updated risk prediction models, personalized care pathways, and integration of cognitive health considerations, the guideline aims to make hypertension control more precise, patient-centered, and outcome-driven.
The Legal Lens
Top 6 Medico-Legal Musts for Every Practitioner
-
Write What You Do, Do What You Write
Your case sheet is your shield. Every examination finding, communication, and consent must be documented in real time, with date, time, and signature. Courts trust contemporaneous records more than memory.
-
Never Treat Without Informed Consent
Always take specific written consent, not generic. Mention the diagnosis, risks, benefits, alternatives, and possible complications. For emergencies, document "implied consent" explicitly.
-
Communicate Compassionately — and Record It
Most medico-legal cases start due to communication gaps, not clinical errors. Record patient/family counselling sessions — date, duration, and what was explained.
If you said it, note it. If you didn't note it, you didn't say it. -
Prescription = Legal Document
Avoid overwriting, abbreviations, or unclear handwriting. Always mention dosage, route, and duration.
If substituting or changing a drug, record why.
Courts consider a prescription equivalent to an affidavit. -
Refer or Consult Early
If a patient is not improving, document timely referrals or telecommunications. Delay in referral is one of the most common grounds for negligence claims.
Write: "Explained need for higher centre / specialist consultation — patient counselled." -
Insure Yourself — Professionally and Emotionally
Professional indemnity insurance is not optional anymore.
Choose one that covers:- Criminal negligence Defense
- Teleconsultation coverage
- Vicarious liability for assistants or staff
Also, remember emotional insurance: support, peer discussion, and counselling when facing litigation.
Interesting Find
Durometer – Essential Tool for Diabetic Footwear Assessment

Durometer - Essential tool for diabetic foot assessment
- Durometer is a device which measures hardness of insoles of footwear.
- It gives measurement in value of shore.
| Hardness | Measurement in shore (°) | Comments |
|---|---|---|
| Ideal | 8-15 | Protect feet Prevent injuries |
| Very soft | <8 | Decrease protection More injury prone feet |
| Very hard | >15 | Increase in callus formation, plantar pressure and ulcers |
Microcellular rubber (MCR) or microcellular polymer(MCP) foot wears are advisable for diabetic foot patients as these have shore of 15° and proven to reduce diabetic foot related complications like callosities ,plantar ulcers etc.
How to use this?
It's a simple non electrical device with small pen tip like sharp end. Sharp end needs to be pressed gently on various parts of footwear especially those who are more prone to excess pressure of feet. One should hold the device for 5-10 seconds steadily to record reading.
This is a simple tool that can be used by Family Physician for footwear education and awareness session or in clinical set up.
AFPI - In the Spotlight

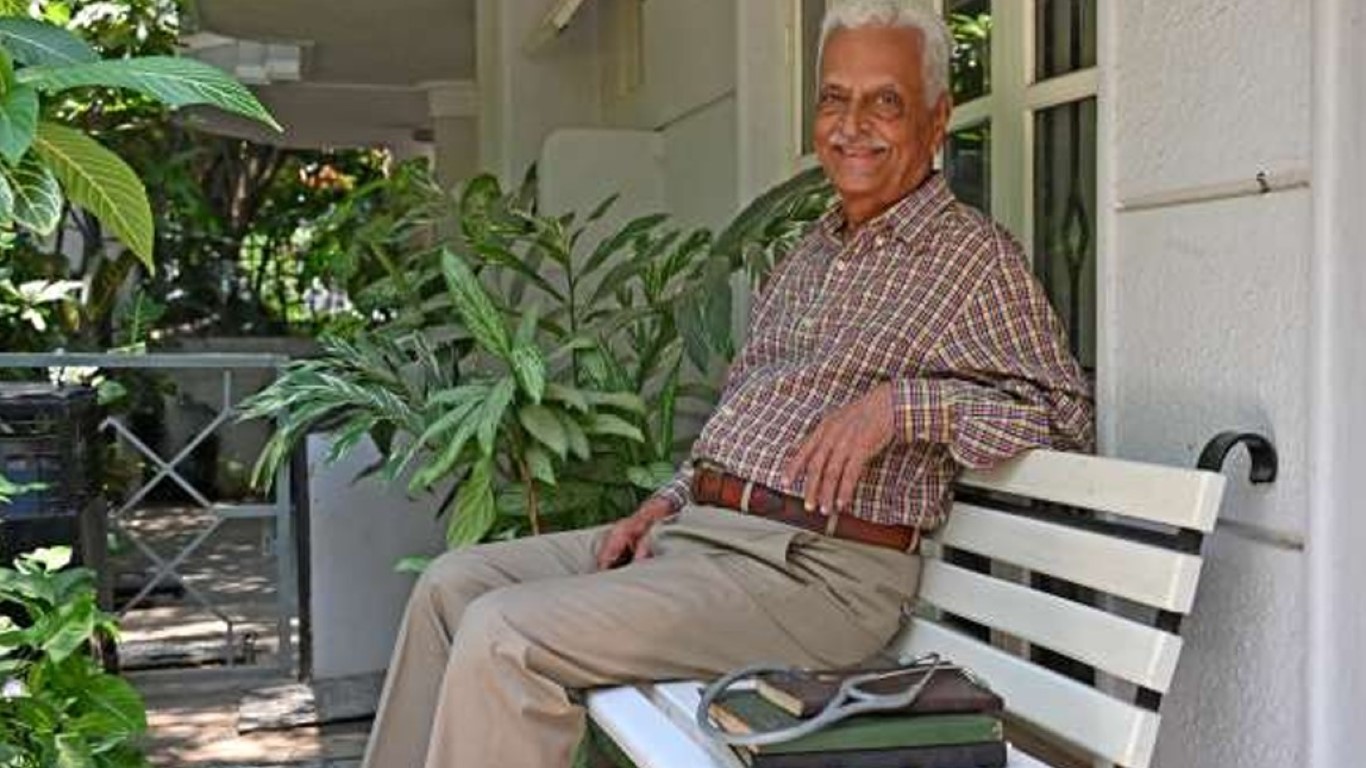
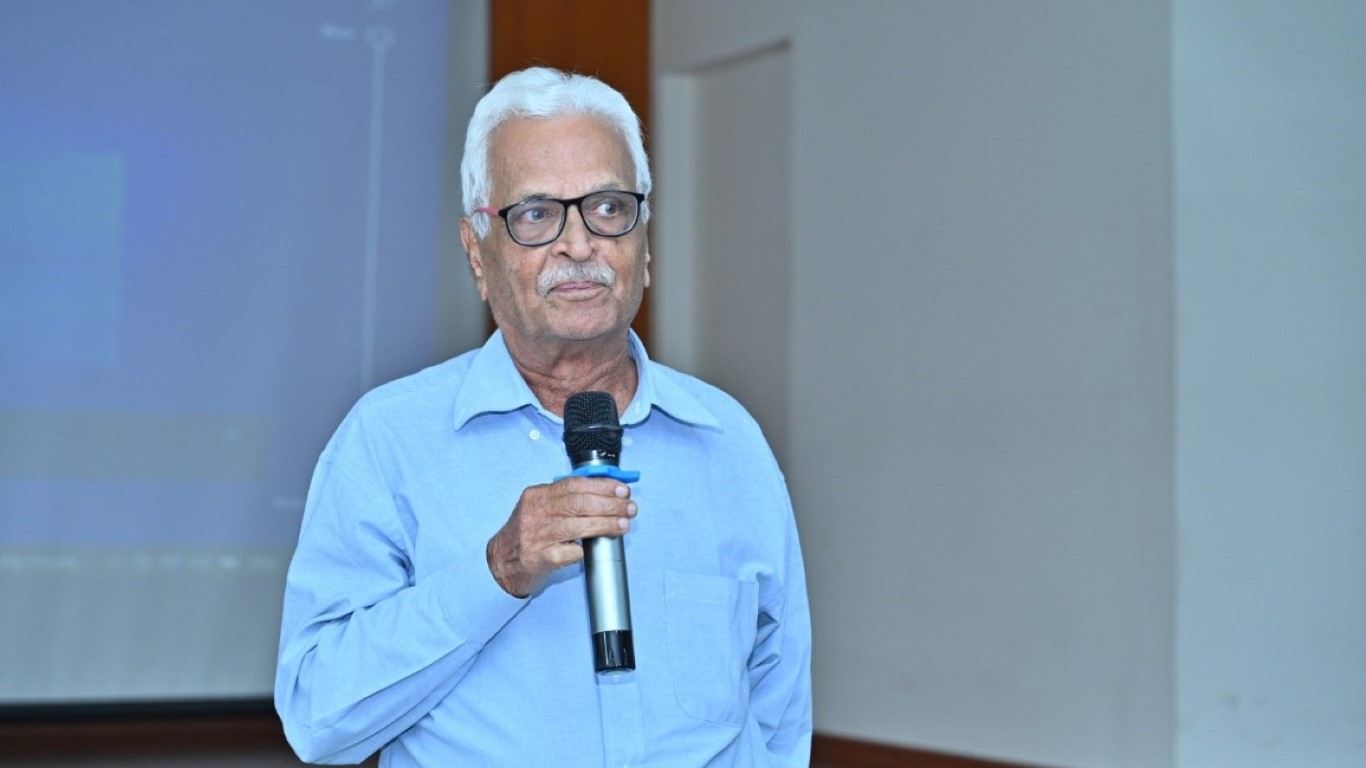
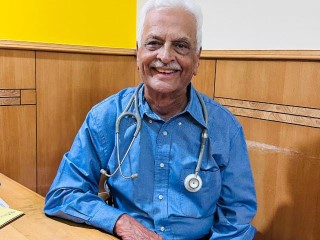
A Living Inspiration – Dr Badekere Rao
It was the summer of 1968 when I set up my practice in a village called Binnamangala in east Bengaluru. The name of the village was eventually lost amid the rapid development around it, and the area came to be known as Indiranagar. I chose Binnamangala because established areas like Jayanagar, Malleswaram, and Basavanagudi already had family doctors, while this emerging locality had only one and I would be the second.
Family medicine now is a bit of a dying practice, and I do not blame younger readers for wondering what it is. It looks after different aspects of health – from preventive and palliative care to treating acute and chronic conditions across ages and sexes, performing minor procedures, supporting mental health, and promoting healthy lifestyles.
Think of us as gatekeepers of health. I encourage patients to keep home-testing kits for blood pressure and glucose, remind women about breast and ovarian cancer screenings, and advise smokers to get chest X-ray examination.
I'm 83 now, semi-retired, and see fewer patients. If not for my habit of keeping a diary of funny yet insightful moments with my patients, many of these memories would have faded with time. I have turned some of these notes — written in Kannada and English — into two books: 'A Family Physician's Life' (2024) and the just-released 'Untold Tales From a Family Physician's Bag'. Family doctors lead interesting lives, and my hope was to share the everyday stories of people's lives through our lens. We stand at the crossroads of healthcare and human connection. Our roles reach beyond the clinic into homes, where we share in both births and losses within patients' families. Our rewards come in many forms — from hugs to tears of joy, bouquets, paintings, and, just this week, a generous batch of Alphonso mangoes!
When I graduated in 1965, India was at war with Pakistan, and the armed forces faced a severe shortage of doctors. Prime Minister Lal Bahadur Shastri appealed to young medical graduates to serve, even briefly. I served as an army doctor for years before setting up practice in Binnamangala, and another one in Cox Town.
Throwback years Before the age of 'Dr Google', patients often came to us uninformed — which was both a boon and a bane. Still, educating them has always been central to our practice, especially for those of us who started half a century ago.
The Changing Face of Medicine
Over the years, I watched healthcare transform. Diagnostics became digital, hospitals became corporate, and the doctor–patient relationship slowly turned transactional. I began to see fewer faces and more files.
Somewhere between the CT scan and the consent form, that human touch — the heartbeat of medicine — began to fade.
Today, I often ask myself: Are we healing the person or merely treating the disease?
Back then, MBBS training was of superior quality, and further study was not essential. Today, an MBBS graduate needs an additional 2 to 3 years of training to become a qualified family doctor. The current education system prioritises specialists, specialists, focusing on curative over preventive care. With fewer family doctors, students have fewer opportunities to observe and learn from — and the field also pays less than most subspecialties. Rarely do hospitals have family medicine as a standalone department. The public is forced to turn to crowded, costly corporate hospitals for even basic care. Staying updated across specialties requires constant study, and I found myself outdated after just three years.
To bridge this gap, doctors like me started the Family Physicians' Association in 1979 and the Doctors Club in 1983 in Bengaluru. Today, I serve as a mentor to the Karnataka branch of the Academy of Family Physicians of India, advocating for primary care's rightful place in India's healthcare system.
Lessons from a Lifetime
In my diary lie hundreds of small stories — a mother's tears when her child's fever finally broke, an elderly man's gratitude after a simple home visit, a young couple's fear during their first pregnancy. These stories shaped me far more than any textbook did.
Each one reminded me that medicine is an art grounded in science — that reassurance and presence often heal faster than prescriptions.
What I Hope for the Future
As I look back, I feel both pride and concern. Pride in the compassion that defined an era of family medicine; concern that in our pursuit of technology, we may forget what truly makes a healer.
I believe it's time to bring back the human touch — to listen more, to see the person beyond the reports, and to remember that trust is still the best therapy.
From My Bag to Yours
These reflections, and many more like them, are what inspired my recent collection,
Untold Tales from a Family Physician's Bag — a mosaic of humour, humility, and heart from my years in practice.
Each story is a reminder that healing begins not in the prescription pad, but in the connection between two human beings — one who seeks help, and one who truly listens.
AFPI Voices

The Power of One Specialty That Embraces All
My experience as EC member, social media head of AFPI Karnataka 2024-2026 & also being part of OC committee of national & international Conference of AFPI was overwhelming.
I would like to begin with; I had a dream of doing a holistic practice which the general medical crowd was at denial. It was a dream come true, reality of being a holistic medical specialist which I had just imagined. I was introduced to family medicine during 2013, which exactly fits into my desire of holistic practice. But there was always a negative side of it, frequently reminded to us by other speciality practitioners about it being less attractive alien speciality lacking regular academic norms. I was naturally searching for a pool of people, an authoritative body who represents family medicine. I met our national & state leaders in 2014-2015 in our Kerala & Karnataka state conference who had so much vision, zeal & enthusiasm as much as I was. This just strengthened my belief & decision of becoming a family medicine specialist, leader & family of AFPI. I found a family of likeminded specialist working with great evidence based scientific knowledge, protocols to build a structured academic training for PG aspirants with NBE. They were also focusing on faculty development programmes in the field of family medicine. Our AFPI association has been constantly encouraging every family medicine specialist & PGs to take a strong lead in Strengthening primary care being part of such activities of AFPI is always a factor of proud. I had received a very optimistic support for actively taking part in organising & heading various committees . Be it as organising secretary, hospitality, social media or cultural committee.
I am just proud & immensely thankful for our national & state leaders for being so dedicated & committed to reach where we are today. I have a sense of belonging; I have a sense of ownership & leadership. I have a sense of responsibly, strong knowledgeable approach to my patients & their family empathetically. I have realised the true sense of who should chose this speciality. Family medicine, is a speciality that has to be chosen by a physician , who wants to be an academically, scientifically, confident, independent leader in primary care. Who doesn't differentiate a systemic approach or any sort of medical challenges. But with unbiased holistic approach treat all kinds of ailments confidently. Assess every system & provide prompt primary care as per standard evidence-based protocol. Prevent the progression or provide continues health care for families of all age group confidently.
My experience with AFPI has always pushed me to be a leader where ever I am.It has provided me a great professional bonding with my senior & junior colleagues. I as a AFPI breed can tell you we have made the Impossible-Possible. We have great team who bring in great ideas & touch new milestones every time we come together. Though we work as a team, I see a leader in each of us giving their best.
My personal strength as I am a family medicine specialist is, I have no boundaries or restrictions of practising in any department. It has genuinely influenced my personal & professional work. I never refused to work with any subspecialities to begin with. I have worked in all departments started with physician in preventive health department, followed by neurology, Gastroenterology, nephrology & cardiology. I have always seen these patients as a whole rather than just a neuro, nephro Or a cardio case. I have managed these cases very well in all aspects including their systemic issue. This has opened multiple opportunity for me. I have my own OPD appointments as consultant family medicine specialist, I work with subspeciality team providing them IP support as junior consultant. I am a clinical safety officer. Also, a trusted physician to whom institution gave an independent hand to manage all normal to critically ill patients during covid & I have been paid appropriately. Have you ever imagined having multiple designation in a same hospital & being paid more than 1salary for each. Today, I can give a health talk anytime on any topic. I can see any patient from OPD to critical case with any systemic illness. I have my own part time clinic in the evening. This privilege has been mine because I am a family medicine specialist. I am taught to be a leader, I am taught to own, innovate & be an artist of Versatility in medical field to support self & work in harmony with another speciality, with continues medical update.
Family medicine students only look forward for having posting in a family medicine department which currently is not possible in tertiary care unit, I believe the whole hospital & every department belongs to us, rather than looking for an isolated department for personal growth which is not possible. Our training is in rotating multiple departments, not restricted to family medicine. keeping this in mind, primary practice has no boundaries, we can enjoy added advantage of Strengthening ourselves post training in family medicine & build our own practice with a strong foundation.
Beyond Medicine

The Other Child: Balancing Love Between the Normal and the Special
This article explores the emotional, psychological, and family dynamics behind illness — beyond prescriptions and medical care.
Back when I watched the movie "Black," I often wondered why the character played by Nandana Sen was so insecure about the one portrayed by Rani Mukherji.
As years passed, and after seeing multiple families face similar situations — and when it eventually struck our own — I began to empathize with Nandana.
When an illness strikes a family, the entire family becomes sick — mentally and physically. When one child is diagnosed with retardation, disability, or a chronic illness, the entire focus naturally shifts to that child. No one notices the other — the so-called normal sibling — who quietly goes through deep emotional and physical struggles too.
It's about being cared for, being the centre of attention, and most importantly, being heard — things often missing in the life of a normal sibling of a diseased child.
What truly matters is being part of the circle — something the normal child is too often left out of. Parents and families must consciously include them in discussions, explain why the diseased child is special, and also remind them why they are equally, if not more, special.
The normal sibling should be encouraged to help — from giving medications to assisting in activities of daily living. Family routines, celebrations, and moments of joy should always include everyone together. The normal child must grow up understanding that having a sibling with a disease is simply the normal of their family.
In the end, it's all about balancing the normal and the abnormal — because in our effort to make the abnormal appear normal, we sometimes forget that the normal may be slowly drifting towards abnormality.
The Last Token
She was the last patient of the day.
The waiting room was empty, the nurses had packed up, and the
doctor was running purely on caffeine and willpower.
She stepped in, smiling. "Just one small doubt, doctor."
He smiled back — every doctor knows that one small doubt is never
small.
Her questions came in clusters: what to eat, what not to, whether stress
really causes acidity, and why her smartwatch keeps scolding her about
sleep.
Ten minutes turned to twenty, and yet neither noticed. Somewhere
between symptoms and side-notes, they laughed. She said she felt
lighter already; he realized his fatigue had lifted too.
When she left, he didn't mark her as the last token.
He just thought — this is why I stayed.
Fun Corner

Word Search Puzzle
Find the following words in the grid:
- HEALTH
- DOCTOR
- PATIENT
- SURGERY
- NURSE
- MEDICINE
- THERAPY
- DIAGNOSIS
- TREATMENT
- VACCINE
Brain Teaser Corner
Family Medicine Crossword • Issue 1
Everyday Clinical Pearls for the Busy Practitioner
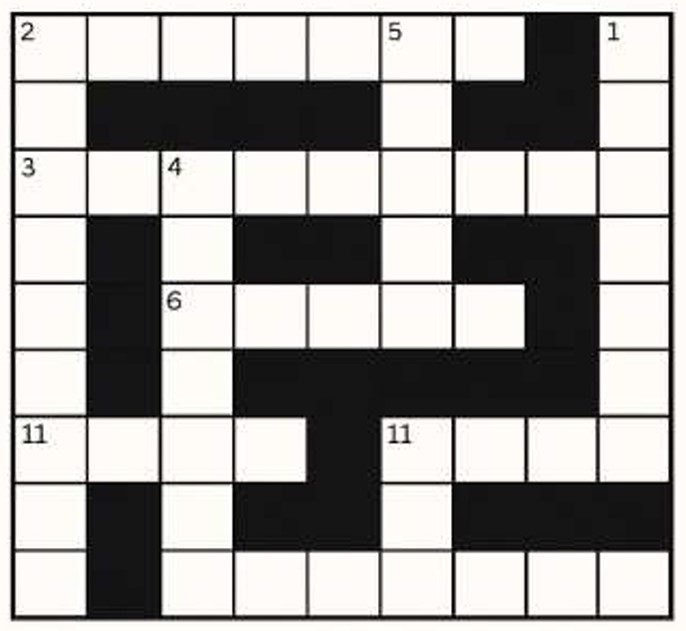
Down
- First vaccine given to a newborn in India
- Diagnostic skin test for TB
- Inhaled drug class used in asthma maintenance
- The "silent killer"
- Commonest bacterial cause of community-acquired pneumonia (10 letters)
Across
- First-line drug for hypertension in diabetics
- Commonest cause of microcytic hypochromic anemia (4 letters)
- Vitamin deficiency causing night blindness (1 letter + 6 letters)
- Mosquito vector of dengue
- Hormone elevated in primary hypothyroidism (3 letters)
- Insulin given IV in DKA
Answers will be revealed in next month's issue.
Reach out to the Editor : doctoraminaa@gmail.com