Messages

Message from the National President - Col (Dr) Mohan Kubendra
As we welcome the New Year, I extend my warm greetings to every member of the AFPI fraternity. The year gone by has been one of purposeful action- strengthening advocacy for Family Medicine, expanding academic initiatives, nurturing young leaders, and reinforcing AFPI's voice at state, national, and international platforms. These achievements reflect your commitment, resilience, and collective spirit.
As we step into the new year, let us renew our resolve to advance comprehensive, person- centred primary care and position Family Medicine at the heart of India's health system. Wishing you and your families a year of good health, professional fulfilment, and shared success.
I am also pleased to share the AFPI National Academic Calendar for 2026, which outlines our planned academic activities and learning opportunities for the year ahead. I encourage all members to actively participate and make the most of these initiatives.

Message from the State President - Dr Sowmya B Ramesh
A very Happy New Year to all the members of the Academy of Family Physicians of India (AFPI), Karnataka Chapter, and colleagues across the country.
The year 2025 was particularly eventful from the Karnataka chapter's perspective, with the successful conduct of an international conference and the privilege of hosting another national conference.
As we move forward into 2026, we propose to begin the year with a physical meet at Baptist Hospital. The primary focus will be on metabolic disorders, highlighting recent updates that are highly relevant to family medicine practice. This academic meet will be hosted at Baptist Hospital.
In addition, we plan to cover several interesting and practical CME topics, including:
- Rabies vaccination: current recommendations and practical issues
- Sarcopenia: understanding and addressing it as we grow older
We also discussed the importance of organizing a Rural CME, as well as continuing AFPI certification programs, details of which will be announced shortly.
Furthermore, we are planning a dedicated "meet and greet" physical gathering — a true break- from- routine CME — where family physicians can come together to deliberate on the growing challenges in family medicine, workplace issues, and evolving career opportunities. This is tentatively being planned as a "Resort CME."
We look forward to your enthusiastic participation and continued cooperation in all these initiatives. Kindly make it a point to attend the morning session and be part of these enriching academic and professional interactions.

Message from Secretary's Desk - Dr Hemavathi
Dear AFPI Members,
Warm greetings to you all and a very Happy New Year! As we step into this new year, I extend my sincere thanks to each one of you for your continued support, commitment, and active engagement with AFPI.
Looking ahead, we have an exciting academic roadmap planned for the coming months. AFPI proposes to organize monthly webinars, quarterly offline CMEs, and a State Conference scheduled for July or August. These academic activities are designed to promote continuous learning, professional growth, and meaningful peer interaction. I encourage all members to make the best use of these opportunities to update knowledge, enhance clinical skills, and stay connected with evolving best practices.
We also warmly invite members to actively contribute to the AFPI newsletter by sharing clinical experiences, interesting case reports, short articles, reflections, or innovations from practice. Your contributions will enrich the newsletter and serve as a valuable learning resource for fellow members.
AFPI strongly believes in member- driven growth. We welcome ideas and suggestions for new academic, clinical, or community- oriented activities, and we encourage members who wish to initiate or lead any activity under the AFPI banner to come forward. Your participation and leadership will shape the future direction of our association.
Let us work together to make this year academically vibrant, professionally fulfilling, and collaborative. I look forward to your active participation and valuable contributions in the months ahead.
From the Editor's Desk

When Medicine Became Too Accurate
Modern medicine has achieved something extraordinary. We now know exactly how much of a drug to give, exactly which number to target, and exactly which guideline to follow. Precision has become our pride. Doses are calculated to the decimal, laboratory values are interpreted to the second digit, and recommendations are neatly boxed into algorithms.
And yet, somewhere along the way, accuracy quietly began to compete with wisdom.
Guidelines were meant to guide, not govern. They are maps, not mandates. But in our anxiety to be "correct," we sometimes forget that maps don't account for traffic, weather, or the fact that the traveller might be limping.
Family physicians see this every day. An elderly patient whose blood pressure is "too low" on paper but perfect for her fragile balance. A diabetic whose sugars are "uncontrolled" yet whose life is finally liveable without hypoglycaemic fear.
The problem is not precision. The problem is reverence. We have begun to treat guidelines like commandments—immutable, unquestionable, and occasionally punitive. Deviation feels like heresy. Clinical discretion requires justification, documentation, and sometimes defence before peers who worship at the altar of protocols.
Ironically, the same fraternity that insists medicine is an art now audits it like an engineering project.
This is where family medicine stands apart. We practise in homes, not just hospitals. We see lab reports in the context of kitchens, finances, family dynamics, and fear. We know that a "borderline" value in a single mother working night shifts is not the same as the same value in a retired executive with a personal chef and a smartwatch.
The future of good care lies not in rejecting evidence, but in softening its edges with context. In knowing when to follow the rule—and when to bend it, responsibly, consciously, and compassionately.
As we step into 2026, I wish every family physician a year of clarity, courage, and calm confidence. A year where we feel less pressured to chase numbers for the sake of compliance, and more empowered to practise medicine that fits the person in front of us.
My goal as editor is to make this newsletter a space for thoughtful, practical, and honest family medicine. I hope it continues to reflect real- world practice—where science, judgment, and lived experience meet.
Wishing all our colleagues a fulfilling, thoughtful, and humane year ahead. Happy New Year.
Academic Commentaries
Pearls from Practice - The Value of Bedside Examination
Dr. B.C. Rao
She had been to other doctors before she visited me. Her complaint was heavy feeling in her abdomen of some year's duration, History and case notes suggested among others, gall bladder stones, stomach cramps, neurosis, and the like. Sheaf of Investigations which included an ultrasound were inconclusive. Ultrasound abdomen showed a retroverted uterus with multiple fibromas with a large one placed posteriorly.
On further questioning she also said gas accumulation and constipation. A Gynaecological check showed a large retroverted uterus with the posteriorly placed fibroma pressing on the rectum and sigmoid colon.
This was the possible cause and as she was 40 plus and perimenopausal she was offered Hysterectomy for which she readily agreed and post- surgery all her complaints disappeared!
A comprehensive physical examination and detailed history taking, even to this day forms the bedrock of patient care. Especially true when one sees the patient for the first time. It takes just 15 minutes to examine the patient head to foot.
If one does not do this one can miss some very important preexisting disease, the patient many not be aware of. Just to illustrate this I will give two more examples which occurred in my practice. The first patient came with some complaints of acid reflux of over many years and has been taking antacids and PPIs, sometimes with prescription and sometimes without. His upper GI endoscopy had shown GERD.
When I saw him as my usual procedure, I found him to be having a hydrocele of the size of a coconut! He surprisingly did not know it was abnormal.
Another patient who has had long standing colostomy bag following surgery for cancer colon came to see me with some abdominal discomfort. Couple of days back. He had been to see a neurologist in a hospital for burning sensations in his feet. Correctly diagnosed as peripheral neuropathy, possibly due to Vit b12 deficiency as it sometimes happens with colostomy patients.
Found him coughing. He had no fever but on examination he was found to have bronchospasm with wide spread rhonchi.
When asked why he did not tell the neurologist he replied, "He did not examine my chest and I thought it was not important." The neurologist did everything right as far as his specialty was concerned but failed to place the stethoscope on the patient's chest to hear the breath sounds.
I would recommend readers to listen to Ted talk by Dr Abraham Verghese on the importance of bedside examination especially in today's practice of medicine which is heavily dependent on labs and imaging and not on bedside history taking and clinical examination.
Drug Update

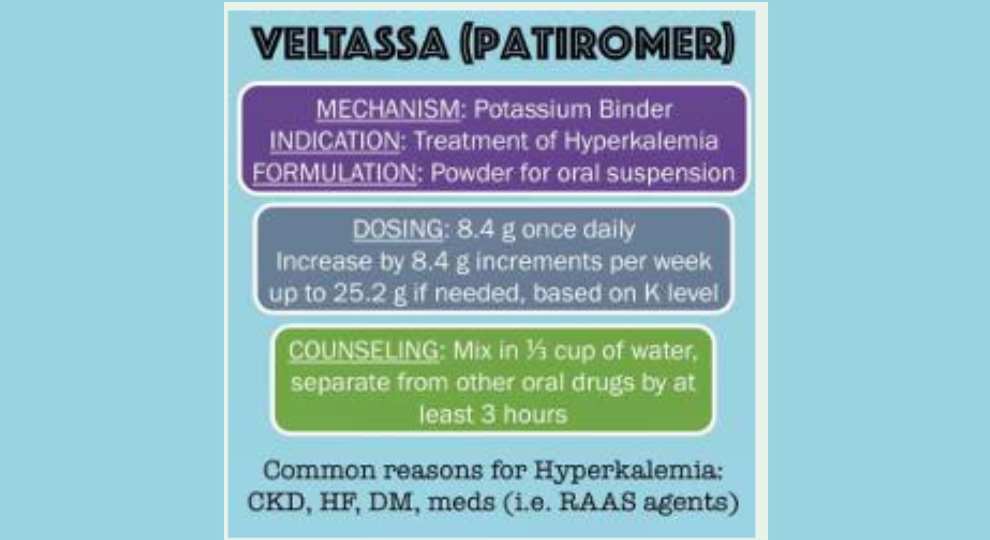
Potassium Control Made Easy: Patiromer in CKD and Heart Failure
Dr. Sowmya B Ramesh
WHY PATIROMER?
- Helps manage chronic hyperkalaemia
- Allows continuation of ACE inhibitors, ARBs, ARNIs, and MRAs
- Safe for CKD stages 3 to 5
- No sodium load, therefore oedema risk is low
HOW IT WORKS
- Exchanges calcium for potassium in the colon
- Increases faecal potassium elimination
- Onset of action: 4 to 7 hours
- Maximum effect: 48 hours
DOSING GUIDE
- Starting dose: 8.4 g once daily
- Titration: Increase by 8.4 g each week
- Maximum dose: 25.2 g per day
Administration instructions: Take with food, Mix in water (do not heat or blend), Separate from other medications by 3 hours.
EXPECTED POTASSIUM REDUCTION
- Lower serum potassium by 0.6 to 1.0 mEq/L
- Up to 90 percent of patients can continue life-saving RAAS therapy
NOT FOR EMERGENCY USE: Patiromer is not for acute or life- threatening hyperkalaemia. It should be used only for chronic, stable potassium control.
SIDE EFFECTS (USUALLY MILD)
- Constipation
- Hypomagnesemia
- Gas or bloating
- Nausea
Avoid use in: Severe constipation, Bowel obstruction
MONITORING
- Check serum potassium 48 to 72 hours after initiation
- Monitor weekly until stable
- Periodically monitor serum magnesium
PATIROMER VS SODIUM ZIRCONIUM CYCLOSILICATE (LOKELMA)
| Feature | Patiromer | Sodium Zirconium Cyclosilicate (Lokelma) |
|---|---|---|
| Onset of action | 4–7 hours | 1 hour |
| Sodium load | No | Yes (may cause oedema) |
| Best use | Chronic hyperkalaemia | Acute and chronic hyperkalaemia |
| Hypomagnesemia risk | Yes | No |
Clinical Pearls:
- Particularly useful in CKD and heart failure patients requiring RAAS inhibition
- Helps avoid discontinuation of ACE inhibitors, ARBs, and MRAs
- Best results when combined with dietary potassium counselling
- Safe for long-term use
Keep hearts strong. Protect kidneys. Control potassium.
Artificial Intelligence & Medicine
Doctor Wars with AI: From Scepticism to Synergy

Doctor Wars with AI: From Scepticism to Synergy
Dr. Syed Mubarak, MBBS, PGDFM, PBDGM, Project Director- Health & Wellbeing, Bosch Global Software
Abstract: The integration of Artificial Intelligence (AI) into medical practice has sparked a debate worthy of a gladiatorial arena, pitting seasoned clinicians against algorithms designed for efficiency and precision. This article explores the evolving relationship between doctors and AI, the tantalizing promise and the vexing challenges.
The year is 2024, and the medical community finds itself in a peculiar sort of cold war. Not against a rival superpower, but against an invisible, yet increasingly ubiquitous, foe (or friend, depending on who you ask): Artificial Intelligence.
The battle lines are drawn not with weapons, but with data points, algorithms, and the occasional exasperated sigh from a doctor struggling to make sense of a new AI- powered diagnostic tool.
Welcome to the "Doctor Wars with AI," a conflict fought not with bloodshed, but with the clinking of keyboards and the quiet whirring of server racks.
Suddenly, the medical world felt a little less like a solo performance and a little more like a duet, with a very advanced, very fast, and sometimes very literal- minded partner.
The AI Advantage: Our Digital Sidekick
Let's be honest, AI has already proven itself to be a remarkably useful sidekick, its ability to process and analyze immense quantities of data has revolutionized:
- Diagnostic Prowess: From detecting subtle anomalies in radiological images that even the most eagle- eyed radiologist might miss, to identifying cancerous cells in pathology slides with unparalleled accuracy, AI has become a powerful diagnostic aid.
- Drug Discovery and Development: The painstaking process of identifying potential drug candidates and predicting their efficacy and safety has been significantly accelerated by AI. Algorithms can sift through millions of chemical compounds in days, a task that would take humans years.
- Personalized Medicine: AI's capacity to analyze individual patient data - genetics, lifestyle, medical history - allows for highly personalized treatment plans. Instead of a one-size-fits-all approach, AI can help tailor therapies, predict responses to medications, dosages, leading to more effective and less toxic treatments.
- Predictive Analytics: AI models can predict disease outbreaks, identify patients at high risk of developing certain conditions, and even forecast patient deterioration in critical care settings.

Detecting subtle anomalies in medical images
The Human Dilemma: Where the Rubber Meets the Road (and the Algorithm)
Despite these undeniable triumphs, the integration of AI isn't always a seamless waltz. Sometimes, it feels more like a clumsy tango with two left feet, particularly when those feet belong to a doctor who's been practicing medicine for decades.
- The "Black Box" Problem: One of the most persistent complaints from clinicians is the "black box" nature of some AI algorithms. AI often struggles to explain why it arrived at that conclusion in a way that a human can readily understand.
Real-Life Example 1: The Frustrated Radiologist. Dr. ABC, a seasoned radiologist, recounts her frustration with a new AI system designed to detect early lung nodules. "It would flag an area as suspicious, but when I asked it why, it would just give me a probability score. It couldn't explain the subtle textural changes/vascular characteristics that a human expert would use to justify their assessment. It felt like it was saying, 'Trust me, I'm an algorithm,' which isn't particularly reassuring when you're dealing with a potentially life-or-death diagnosis."
The lack of transparent reasoning can erode trust and hinder learning.

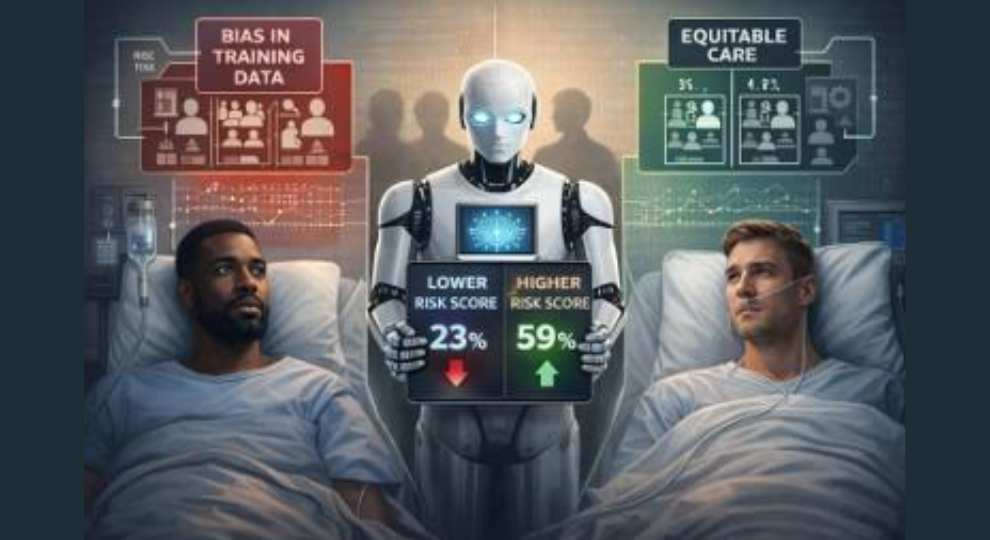
- Data Bias and Ethical Concerns: AI systems are only as good as the data they are trained on. If the training data is biased, the AI will perpetuate and even amplify those biases, leading to inequitable healthcare.
Real- Life Example 2: The Underrepresented Patient. A study published in Science in 2019 revealed an AI algorithm used by a major health system disproportionately assigned lower risk scores to Black patients, leading them to receive less medical attention than equally sick white patients.
This wasn't due to explicit racism in the algorithm's code, but because the training data reflected existing societal biases in healthcare access and utilization. This highlights a crucial ethical dilemma: are we inadvertently hardwiring prejudice into our healthcare systems?
- The Loss of the "Art" of Medicine: Many doctors worry that an over- reliance on AI could lead to a decline in critical thinking and clinical intuition - the intangible "art" of medicine.
Real- Life Example 3: The Overly Reliant Resident. Dr. XYZ, an internal medicine attending, observed a resident meticulously following an AI- generated treatment plan for a complex patient, even when the patient's presentation subtly diverged from the AI's predicted course.
"The resident was so focused on the AI's recommendations that he almost missed a crucial change in the patient's mental status that wasn't immediately flagged by the system. He was treating the algorithm, not the human being in front of him. We need to remember that AI is a tool, not a replacement for clinical judgment." The human element of empathy, communication, and holistic understanding remains paramount.

- Implementation Hurdles and Integration Woes: Adopting new AI technologies often comes with significant IT infrastructure challenges.
Real- Life Example 4: The EHR Headache. A new AI- powered electronic health record (EHR) system designed to optimize workflows and reduce charting time. The rollout was plagued by technical glitches, incompatible legacy systems, and a steep learning curve for hundreds of physicians and nurses. "It felt like we were back in medical school, learning a whole new language," lamented Dr. Sarah Jones, a pediatrician. "The promised efficiency gains were completely overshadowed by the hours spent troubleshooting and entering data into a system that was supposed to make our lives easier."
The Way Forward: Synergy, Not Supremacy
The "Doctor Wars with AI" are not about one side winning and the other retreating in defeat. This isn't a zero- sum game. The future of medicine lies in a synergistic partnership.
We must become discerning users, critical evaluators, and ethical collaborators with AI, while we, the human physicians, bring the wisdom, the empathy, and the nuanced understanding of the individual to make the ultimate, informed decisions for best outcomes overall.
Practice & Perspective

Abnormal Uterine Bleeding (AUB): A Practical Approach for the Primary Care Physician
Dr. Krithika Ganesh, MBBS, DNB (Family Medicine), Consultant Family Physician, The Pocket Family Doctor Clinic, Bangalore
Why AUB Matters in Primary Care
Menstrual disorders account for nearly one in five visits by women especially in their reproductive years to a doctor. The family physician is often the first point of contact—making skill of a structured evaluation important.
Normal menstrual parameters (FIGO): Cycle length 24-38 days, duration 4.5-8 days, volume 5-80 mL (helps the patient to quantify heavy/ scanty bleeding based on her previous normal cycles).
Any deviation from these norms qualifies as Abnormal Uterine Bleeding (AUB). Please note that AUB is a symptom, not a diagnosis!
A Practical Approach for Primary Care
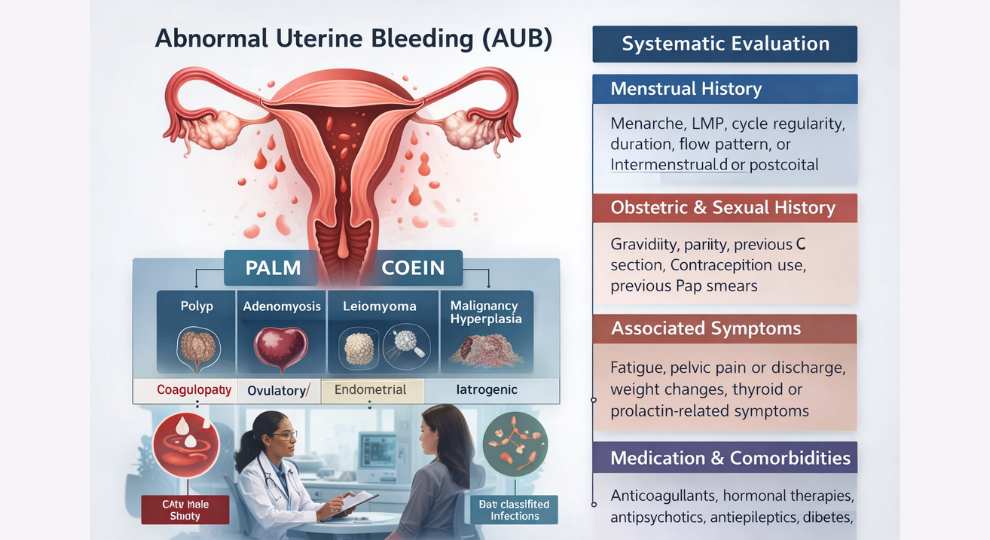
The FIGO Classification (PALM- COEIN)
The FIGO system classifies AUB into structural and non- structural causes:
- Structural (PALM): Polyp, Adenomyosis, Leiomyoma, Malignancy and Hyperplasia
- Non- structural (COEIN): Coagulopathy, Ovulatory dysfunction, Endometrial causes, Iatrogenic, not yet classified (AV malformations, infections)
Multiple causes often coexist in a single patient. Hence, a systematic stepwise approach is key to arriving at a diagnosis.
History: The Heart of Diagnosis
AUB evaluation starts with a detailed history, which often guides the rest of the workup.
- Menstrual History: Menarche, LMP, cycle regularity, duration, flow pattern, intermenstrual or postcoital bleeding
- Obstetric and Sexual History: Gravidity, parity, previous C section, contraception use, previous Pap smears
- Associated Symptoms: Fatigue, pelvic pain or discharge, weight changes, thyroid or prolactin- related symptoms
- Medication & Comorbidities: Anticoagulants, hormonal therapies, antipsychotics, antiepileptics, diabetes, hypertension, PCOS, thyroid disorders
- Family History: Coagulopathy or malignancy (breast, ovarian, endometrial, colon)
Screening with History for Bleeding Disorders
Up to 13% of women with heavy menstrual bleeding have an undiagnosed coagulopathy. A screening history (90% sensitivity) includes:
- Present since menarche?
- One of the following: previous postpartum hemorrhage? surgical related bleeding? dental- related bleeding?
- Two or more of the following: bruising at least 1- 2 times a month? Nose bleeds 1- 2 times a month? frequent gum bleeding? a family history of bleeding symptoms?
Examination and Investigations
Physical Examination: Pallor, BMI, signs indicating thyroid disease, hirsutism, abdominal/pelvic masses, cervical lesions
Baseline Investigations: CBC, Ferritin, Urine/Serum β-hCG, TFT, Prolactin, Coagulation screen, Pelvic ultrasound, Pap smear
Indications for endometrial biopsy:
- In all women >40 yr with AUB
- In women < 40 yr with high risk factors of Ca endometrium such as:
- Endometrial thickness >12 mm on USG
- AUB unresponsive to medical treatment
- Obesity, PCOS, Diabetes, hypertension, GB or thyroid disease
- Family history of malignancy of ovary/breast/endometrium/colon
- Tamoxifen treatment
- Nulliparous
- History of infertility
Case 1: The Adolescent with Heavy Bleeding
Ms. P, 13 years, presents with prolonged, heavy periods for 6 months. Pads soaked hourly, each cycle lasting 10 - 12 days, fatigue, missing school days. Examination shows pallor but otherwise unremarkable.
Based on history in this age group we can think of these likely causes: Anovulatory cycles (immature HPA axis), PCOS or thyroid dysfunction, Coagulopathy. (Structural causes are more common in perimenopausal age and should be first suspected in that age group).
Workup: CBC, UPT/ serum β-hCG (with consent), Thyroid function test, serum Ferritin, Coagulation screen (if suspected).
*Note that in this age group an ultrasound imaging would be indicated only if there are specific findings on physical examination that point to a structural cause. Nonstructural causes are commonly seen in this age group.
Management:
Non-Hormonal
- Tranexamic acid 15-25 mg/kg 2-3 times daily (max 1 g)
- NSAIDs (Mefenamic acid 500 mg TDS, Naproxen 250-500 mg BD)
- Iron supplementation
Hormonal treatment
To stop acute bleed: Norethisterone 5- 10 mg TID for 5- 10 days then weaned slowly or medroxy- progesterone acetate 10- 20 mg TID for 10 days then weaned.
(Please note: progesterone- only treatment if stopped abruptly will precipitate bleeding)
If recurrent, consider Cyclical OCPs - low dose estrogen and progestin (e.g. ethinylestradiol 30 mcg + levonorgestrel 150mcg) cyclically useful for irregular and anovulatory cycles.
Age-based Approach to AUB
13- 18 yr old:
- Ovulatory (AUB - O) due to immature HPA axis/ anovulation
- Androgen excess / obesity/ PCOS/ thyroid disorders
- Coagulopathies
19 - 39yr old:
- Pregnancy
- AUB-O - PCOS, thyroid disease, hyperprolactinemia, stress, intense exercise, eating disorders
- Structural lesions
- Iatrogenic - OCPs, IUD, medications
- Endometrial hyperplasia
>40 yr old:
- Structural lesions
- Endometrial Hyperplasia
- Ovulatory dysfunction due to declining ovarian reserve/perimenopause
- Endometrial CA
Case 2: The Perimenopausal Woman with Fibroids
Mrs. H, 45 years, G3P3L3, reports progressively heavy menses over past 1 year and dysmenorrhea. It is accompanied by fatigue and frequent loss of work days. Examination and Investigations: Pale, uterus 14- week size. USG: Two large fibroids. Endometrial biopsy: Negative. Hb: 8.6 g/dL, low ferritin.
Approach: Endometrial Biopsy is recommended in all women with AUB above 40yr age.
Management options:
- Medical: Tranexamic acid, NSAIDs, Iron therapy
- Hormonal: LNG-IUS (Mirena), progesterone only pills, GnRH agonists
- Surgical: Myomectomy or hysterectomy depending on symptoms, size and patient preference.
Wrapping up AUB in Primary care:
Primary care doctors play a pivotal role in:
- Early recognition and classification using FIGO systems
- Ruling out pregnancy, coagulopathy and other systemic causes such as thyroid disease.
- Initiating first-line therapy and correcting anemia
- Recognizing red flags for referral (malignancy, hemodynamic instability)
With structured evaluation and empathetic counselling, we can make a big difference in women's health outcomes.
Key Takeaways
- AUB is a symptom, not a diagnosis
- Always remember to rule out pregnancy first in all women of reproductive age group
- History + targeted investigations = 80% of diagnosis
- Routine Ultrasound imaging not required in adolescent AUB unless there is a suspicion of structural causes
- Suggest endometrial biopsy in all AUB >40yr and those <40 with risk factors
- Avoid outdated terms like menorrhagia, metrorrhagia, DUB etc. Apply FIGO PALM-COEIN classification instead.
- Family physicians can manage AUB cases effectively at the primary level with empathy and systematic clinical approach.
References
- Wouk N, Helton M. Abnormal Uterine Bleeding in Premenopausal Women. Am Fam Physician. 2019;99(7):435-443.
- Jain V, Munro MG, Critchley HOD. Contemporary evaluation of women and girls with abnormal uterine bleeding: FIGO Systems 1 and 2. Int J Gynaecol Obstet. 2023;162 Suppl 2:29-42.
- FOGSI Recommendations - Evidence-based management of AUB in the reproductive age group.
Case Reports
Young Guns Fire - Poster Presentation from the Young Brilliant Generation
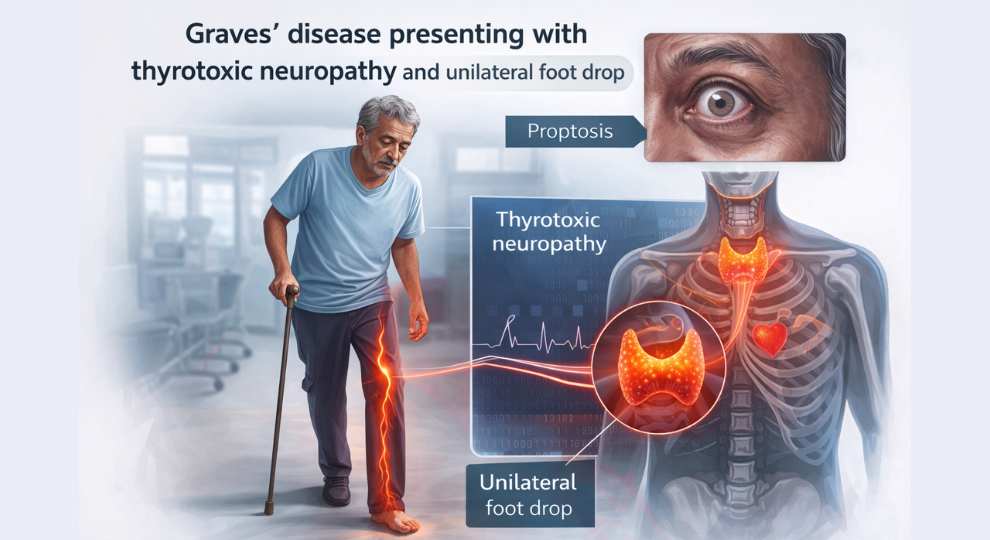
Beyond Tremors and Weight Loss: Atypical Neuromuscular Presentation of Graves' Disease
Dr. Syed Mohammed KA, Dr. Hemavathi D, Department of Family Medicine, St. John's Medical College, Bangalore, AFPI – Karnataka Chapter
Introduction
Hyperthyroidism commonly presents with weight loss, palpitations, and tremors. However, neuromuscular manifestations of hyperthyroidism, though less common, include: Ophthalmopathy, Periodic paralysis, Myasthenia gravis, Thyrotoxic myopathy.
Atypical neurological presentations may delay diagnosis if thyroid disease is not considered early.
Case Presentation
Patient Profile: 53-year-old male farmer
Presenting Complaints:
- Chronic diarrhoea for 1 month
- Unintentional weight loss (~6 kg in 1 month)
- Progressive bilateral lower-limb weakness for 20 days
- Difficulty lifting the front part of the right foot while walking (20 days)
Psychosocial Context:
- Ideas: Fear of a serious or irreversible illness
- Concerns: Inability to work, financial stress, increased dependence
- Expectations: Regaining strength and resuming farming activities
Clinical Examination
General Examination: Anxious appearance, warm skin, fine tremors, No goitre, Pulse: 106 bpm, irregularly irregular, Blood Pressure: 130/80 mmHg
Neurological Examination:
Motor System: Bulk: Normal, Tone: Normal, Power: Bilateral hip flexors & extensors - Grade 3/5, Right ankle dorsiflexion - Grade 3/5
Reflexes: Deep tendon reflexes: Brisk, Babinski sign: Negative
Sensory System: Normal
Gait: Right- sided high- stepping gait (foot drop)
Investigations
Thyroid Function Tests:
- TSH: < 0.0025 mIU/L (Decreased)
- Free T4: >5 ng/dL (Increased)
- Free T3: >20 pg/mL (Increased)
- Anti- TPO antibodies: >1000 IU/mL (Positive)
Thyroid Scan (99mTc- Pertechnetate): Enlarged thyroid with diffusely increased uptake, Total uptake: 11.4% (Normal: 0.3 - 3%), Reduced uptake in right lower pole, Suggestive of diffuse toxic goitre (Graves' disease)
Nerve Conduction Study: Bilateral motor axonal neuropathy (Right > Left), Sensory sparing
ECG: Atrial fibrillation
Diagnosis
Graves' disease presenting with thyrotoxic neuropathy and unilateral foot drop
Treatment
- Carbimazole
- Propranolol
- Physiotherapy
Follow- Up (After 4 Weeks)
- Muscle power improved to Grade 4+/5
- Foot drop: Improved
- Diarrhoea: Resolved
- Heart rate/ECG: Normal sinus rhythm
- TSH increased from <0.0025 to 0.04 mIU/L
- Free T4 decreased from 4.43 to 1.01 ng/dL
The patient regained muscle strength and resumed daily activities.
Discussion
Based on clinical features and laboratory findings, a diagnosis of Graves' disease was established. Unilateral foot drop is most commonly caused by peroneal nerve injury, radiculopathy, or compression. Thyrotoxicosis presenting as foot drop is a rare manifestation. Early recognition and appropriate antithyroid treatment can lead to complete neurological recovery, highlighting the reversibility of this condition.
Conclusion
After excluding common causes, thyrotoxicosis should be considered as a differential diagnosis in patients presenting with foot drop, especially when accompanied by other symptoms of hyperthyroidism. Early diagnosis and treatment of Graves' disease can result in significant neuromuscular recovery. Family physicians play a key role through symptom-directed evaluation, early treatment, and timely referral.
Learning Points
- Endocrine disorders, particularly thyrotoxicosis, can present with neuromuscular symptoms.
- Diarrhoea and foot drop may be the sole manifestations of Graves' disease.
- Anti-TPO positivity supports an autoimmune aetiology, and early treatment is often rewarding.
References
- Garces-Sanchez M, Alvarez-Tejado M, Esteban J. Neuromuscular complications of thyrotoxicosis: A review. Rev Neurol. 2000;31(6):543-548.
- McComas AJ, Sica RE. Neuropathy associated with thyrotoxicosis. J Neurol Neurosurg Psychiatry. 1969;32(6):643-647.
- Hara K, Miyata H, Motegi T, Shibano K. Thyrotoxicosis presenting as unilateral foot drop. Intern Med. 2017;56(15):2053-2056.
An Emerging Neurological Concern
District Hospital Vijayapura - Brain Health Clinic
Presenter: Dr. Sajida Yaligar (Intern)
Guide: Dr. Bharath Sarguru (Senior Resident), District Hospital Vijayapura, AFPI - Karnataka Chapter
Introduction
Migraine is a common primary headache disorder that increasingly affects adolescents and young adults. It is often underdiagnosed and undertreated, leading to impaired academic performance, reduced productivity, and poor quality of life in the younger population.
What Is Migraine?
Migraine is a primary headache disorder characterized by recurrent attacks of moderate to severe headache, typically: Unilateral, Pulsating or throbbing in nature, Associated with nausea, vomiting, photophobia, and phonophobia.

Epidemiology
- Second most common cause of headache worldwide
- Affects approximately 12% of the general population
- More common in females (female: male ratio ~ 3:1)
- Onset usually during adolescence or early adulthood
- Peak prevalence between 30–39 years of age
Clinical Features
Prodrome: Yawning, Mood changes, Food cravings
Aura (if present): Zigzag lines, Scotoma, Sensory disturbances
Headache Phase: Unilateral, Throbbing pain, Moderate to severe intensity, Duration: 4–72 hours, Associated with nausea, vomiting, photophobia, and phonophobia
Postdrome: Fatigue, Difficulty concentrating
Pathophysiology
- Activation of the trigeminovascular system leading to neurogenic inflammation
- Cortical spreading depression (CSD) associated with aura
- Serotonin (5-HT) dysregulation plays a major role
- Calcitonin Gene–Related Peptide (CGRP) contributes to vasodilation and pain transmission
Types of Migraine
- Migraine without aura (Common migraine) - Accounts for approximately 75% of cases
- Migraine with aura (Classic migraine) - Accounts for approximately 25% of cases. Aura refers to transient visual, sensory, or speech disturbances that precede the headache.
Migraine vs Tension-Type Headache
| Feature | Tension-Type Headache | Migraine |
|---|---|---|
| Pain character | Mild to moderate, tightening or band-like | Unilateral, throbbing |
| Frequency | Variable | ≥ 5 episodes |
| Aura | Absent | May be present |
| Duration | Variable | 4-72 hours |
Simplified Diagnostic Criteria for Migraine
Recurrent headache attacks lasting 4-72 hours in patients with a normal physical examination and no other reasonable cause, AND:
At least 2 of the following: Unilateral pain, Throbbing quality, Moderate to severe intensity, Aggravation by routine physical activity.
Plus, at least 1 of the following: Nausea and/or vomiting, Photophobia and phonophobia.
Conclusion
Migraine is a significant and emerging neurological problem among younger individuals. Early recognition, accurate diagnosis, and appropriate management can significantly improve quality of life and prevent long- term disability.
References
- Diagnostic and treatment protocol for neurological disorders for secondary health centres. Karnataka Brain Health Initiative, Bangalore: NIMHANS.
- Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, Holland S, Langford C. Harrison's Principles of Internal Medicine, 22nd ed. McGraw- Hill Education; 2025.
Benign Recurrent Intrahepatic Cholestasis Presenting as Fatal Intracranial Haemorrhage in Pregnancy – A Case Report
Lijo Joseph1, Ashiqque Ali NK2, Senior Resident, Emergency Medicine Critical Care, St. John's Medical College Hospital, Bangalore – 560034, AFPI – Karnataka Chapter
Introduction
Benign Recurrent Intrahepatic Cholestasis (BRIC) is a rare genetic disorder characterized by recurrent episodes of intrahepatic cholestasis, presenting with intense pruritus and jaundice. During pregnancy, cholestasis can lead to coagulopathy secondary to vitamin K malabsorption, increasing the risk of maternal and foetal bleeding complications.
Intrahepatic cholestasis of pregnancy (ICP) is a pregnancy- specific liver disorder causing pruritus and elevated bile acids, with potential adverse maternal and foetal outcomes. Although BRIC is generally considered benign, pregnancy can act as a trigger, and overlap with ICP may complicate management.

Aim of the Study
To emphasize the importance of early suspicion, timely referral, and comprehensive management of Benign Recurrent Intrahepatic Cholestasis (BRIC) during pregnancy, particularly in preventing rare but catastrophic complications such as fatal intracranial haemorrhage.
Methodology
Clinical data were obtained and analysed from medical records and patient attendants, with written informed consent from the family and the primary treating physician.
Case Report
A 28- year- old pregnant woman (G2P1L1) with a known history of Benign Recurrent Intrahepatic Cholestasis (BRIC) presented at 34+5 weeks of gestation. She had undergone a previous caesarean section 11 months earlier. She had been recently started on Ursodeoxycholic acid and Rifampicin, along with routine antenatal medications.
First Trimester:
- Pregnancy was unrecognized until 22 weeks
- At 11 weeks: Total bilirubin: 2.9 mg/dL, Direct bilirubin: 2.06 mg/dL, AST: 58 IU/L, ALT: 32 IU/L
- Rifampicin 150 mg twice daily initiated
Second Trimester:
- Ursodeoxycholic acid added at 20 weeks
- 22-week anomaly scan: Normal
- Received tetanus vaccination, iron, and calcium supplementation
- OGTT: Normal
- At 26+5 weeks: Total bilirubin: 2.95 mg/dL, Direct bilirubin: 2.39 mg/dL
- Ursodeoxycholic acid increased to 300 mg twice daily
Third Trimester:
- At 31+5 weeks: Developed generalized pruritus, Admitted and treated, TB: 3.4 mg/dL, DB: 2.6 mg/dL, Rifampicin dose increased, Received two doses of betamethasone, Discharged after symptomatic improvement
Current Admission (34+5 weeks): Presented with headache and vomiting, Vitals: Stable, Pallor and icterus present, Per abdomen: 34 weeks, cephalic presentation, Uterus relaxed, foetal heart rate present, Other systems: Normal.
Within 12 hours of admission, the patient became drowsy and suffered cardiac arrest. Return of spontaneous circulation (ROSC) was achieved.
An emergency caesarean section was performed, delivering a live female infant: Apgar score: 3 and 6, Birth weight: 2.216 kg, Admitted to NICU.
The mother was shifted to Critical Care postoperatively. Despite intensive ICU management, the patient succumbed on day 3 of admission.
Investigations
- Liver function tests: Deranged
- Prothrombin time and INR: Mildly elevated
- Leucocytosis with neutrophilic predominance
CT Brain Findings: Intraparenchymal haemorrhage in the right cerebellar hemisphere, Active bleeding with diffuse cerebral oedema, Likely secondary to cerebral venous thrombosis (CVT), Trans tentorial herniation with supratentorial hydrocephalus.
Discussion
Family physicians are often the first point of contact for pregnant women and must maintain a high index of suspicion for bleeding manifestations in patients with BRIC or intrahepatic cholestasis.
Delayed diagnosis and management can result in severe and fatal outcomes. Evidence suggests that intrahepatic cholestasis of pregnancy can cause coagulopathy due to impaired vitamin K absorption, leading to life- threatening haemorrhage.
Pathophysiological Sequence
- Liver disease / BRIC / Cholestasis
- Impaired bile excretion
- Poor fat and vitamin K absorption
- Vitamin K deficiency
- Coagulopathy (prolonged INR/PT)
- Increased maternal and foetal bleeding risk
Prophylactic vitamin K supplementation should be considered in patients with ICP and BRIC to mitigate catastrophic outcomes.
This case underscores that ICP with coagulopathy is an obstetric emergency, necessitating multidisciplinary collaboration and heightened clinical vigilance.
Conclusion
Benign Recurrent Intrahepatic Cholestasis is characterized by recurrent cholestatic episodes and, though typically benign, can lead to fatal complications during pregnancy. Clinicians must remain vigilant for this condition, particularly when triggered by pregnancy. Early suspicion, proactive management, and multidisciplinary care are crucial in preventing devastating maternal outcomes.
References
- Gelardi E, Vulliamy N, Graham J, Kourouclis D, Sevastianos V, Alexopoulou A. Benign Recurrent Intrahepatic Cholestasis: Where Are We Now? Gastroenterology Research and Practice. 2024;15:56-67.
- Maldonado M, Alhusseini A, Awadalla M, Idler J, Wieck R, Puder K, Pawchand M, Gorki B. Intrahepatic Cholestasis of Pregnancy Leading to Severe Vitamin K Deficiency and Coagulopathy. Case Reports in Obstetrics and Gynecology. 2017;2017:5646427.
- Sultana J, Komai M, Shirakawa H. The Role of Vitamin K in Cholestatic Liver Disease. Nutrients. 2021;13:2551.
Why Honest Conversations Matter

Opening the Curtain: Why Honest Conversations Matter in Family Medicine
Dr Madhavi, Pioneers into the Pain Management Sphere - Palliative Medicine
An elderly man lay in his room while his family stood outside, worried. They asked the doctor to keep the curtains drawn so the man would not see the dark clouds gathering outside. "If he sees the storm," they said, "he will lose hope."
The doctor gently opened a small part of the curtain. The man looked out, saw the clouds, and said, "I knew the weather was changing. Thank you for letting me see. Now I can decide whether to stay inside, call my children closer, and rest."
The storm did come—but the man was no longer in the dark.
In Indian family practice, doctors often work within close- knit families where health decisions are shared and family members play a central role in care. It is therefore common for families to ask that the diagnosis, prognosis, or seriousness of illness be withheld from the patient, hoping to protect them from emotional harm. This practice, known as collusion, usually arises from love and fear rather than ill intent. Breaking collusion in this setting means gently and compassionately sharing the truth with the patient, while remaining sensitive to family values and concerns.
For family physicians and palliative care providers, this step is essential—not only to uphold patient dignity, but also to open the door to meaningful conversations about goals of care, future planning, and end- of- life preferences.

Open communication is central to good family medicine practice. When collusion is addressed with sensitivity and respect, patients are able to understand their illness, participate in decisions, and express their values and preferences. Families, in turn, are better supported and less burdened by uncertainty or later regret.
Honest conversations—held with empathy and cultural awareness—do not take away hope; they enable preparedness, trust, and care that is truly patient- centred. By choosing to gently open the curtain, family physicians play a crucial role in guiding patients and families through illness with clarity, dignity, and compassion.
Holding the Ground

Holding the Middle Ground
Dr. Priti Shankar, Academic chair FFPAI, Family Physician
Family physicians don't just treat disease. They witness, Children becoming caregivers. Financial collapse due to chronic illness. Cultural conflict around decision- making. Not every illness shows up in a blood report. Some sit quietly across the table, masked as routine follow- ups, speaking only through tired eyes and long silences. What began as an ordinary diabetes consultation slowly revealed a truth every physician eventually learns—that sometimes, the deepest healing has nothing to do with medicines at all.
This was one of my friends rather regular patient who became a friend! She has come to me in the beginning for uncontrolled diabetes!
A widow for 3 years living with her elder son (who was a spinster by the way) since her husband's demise! This son of hers was a nice person taking good care of his mother but not of himself which was seen in his looks! Untrimmed beard shuffled hair and always stressful look!
I used to reassure him that his mother was doing well and her sugars will surely be totally under control soon! He smiled briefly and said he was confident that she will be fine but his stress continued. I checked if it was financial problem I could adjust his mother's medication! He said finance was not at all and issue and no further discussions on those lines!
Weeks passed few months passed she was brought to me by a younger person. He introduced himself as her younger son as his brother expired suddenly! He had come down to take his mother to Chennai after the rituals! My patient was silent with tears flowing and was too shaken even after a month of her son's death.
I let it be changed her medicines as required and told her to meet my classmate in Chennai for follow up! It was indeed a sad day for me. But life goes on and probably will be the same with her too!
She was back after a few months this time wanted to meet me to show her regular blood reports! Still the silent lady with drooping eyes close to tears all the time except the brief smile when she entered my chamber ! Her reports were fine and very minor adjustments to medication and that would have been end of my consultation.
But I continued to talk to her advised her to move on and live with her son's fond memories! She cried more and started talking a little! I went on and then she said that her daughter in law doesn't like her and she can't live with her! Then the son told his part of the story that he had 2 children and his wife had never lived with her earlier and found adjustment difficult!
Sensitive topic so I kept out for a while and then very hesitantly told her to find other options of staying! Many senior living centres where she can be more comfortable and lo her eyes brightened! I can live alone doctor but not where I have no respect! Very embarrassing for her son, it was and I understood his situation too.
I explained to her that as children grow up their responsibilities and priorities change and rightfully so! I gave them the contact numbers of some senior living homes and saw her face brighten up and they both left happily thanking me! Son expressed a special thanks to me for explaining to her his situation too which he was unable to do!
What would have been a 10 to 15 minutes consultation Max took almost 45 minutes but in the end was truly rewarding. The smile and relief on both their faces and her hug was not a small thing in the midst of my practice!
The Move - Across the Borders

The Move: Crossing Borders: A Career in the UK
Dr Ramya, MBBS, DNB Family medicine, MRCP- Internal medicine, MRCGP
It is an absolute honour to write a column in the AFPI newsletter!!
I have been a GP all my life, starting from when I qualified with a DNB in Family Medicine in 2012 from The Bangalore Hospital at South End Circle. As with many doctors, one degree didn't satisfy my scholarly pursuits and so went on to do MRCGP [Int]. One should think that's more than enough but circumstances lead me to getting one more degree and probably, the last one, MRCGP [Uk]. So, that's my credentials, which means I know the exam systems in 2 countries pretty clearly.
What made me move to Uk?
I'd like to think it's destiny. I was in a comfortable job in India, working with the most spectacular team and building a Family medicine set up with a well- funded start up. All good things come to an end and this start up ended with Covid. However, I had left India in 2019, a year before Covid. Coming back to the destiny, one day in 2016, an ad came up for a GP job in Uk, the requirement was DNB and MRCGP Int, so I applied for it and was successful, they offered me the job !
The next part was to apply for something called the CEGPR (a common equivalent would be CESR route for other specialities), it's a way for GMC (General Medical Council) to recognise your qualifications as equivalent to a GP trained in Uk.
After sending 4kgs of supporting paper work, spending 1.5 lakh Indian rupees and waiting for 11 months, I got a rejection. Reason, I was not trained in Uk or EU and did not have work experience in any of these said areas. Now, that was pretty clear in my application so they could have rejected it immediately, but no, that's the British way, everything takes forever. Take note, you will hear about the endless patience that British folk have in my articles to come.
I had never actively looked for jobs in Uk or made plans to move before this job came up, but in the ensuing 11 months, me and my family (husband and then 9- year- old daughter), had completely made up our minds about moving to Uk. The excitement in our house in those days was amazing, researching about houses, schools, expenses in Uk, all done and ready. So, when the rejection came, it was an absolute gut wrenching ,heart sink moment.
On a side note, my husband worked in the IT industry, as most people in Bangalore ! And his job required him to travel to Europe very often so, a move to Uk would be perfect for us. I was just not willing to give up on the dreams we had built together, so I decided to look for ways to get to Uk.
The Journey to UK
I started working on writing PLAB, got through the first part, which is a straight forward MCQ exam. Went to Uk for part 2 with the family, had a 2- week vacation there, to really help us make up our mind on whether we wanted to move or not.
Part 2 is a simulated practical exam with 18 stations. You will have to consult with patients, do procedures and deal with emergencies on 'Sim man', a simulated mannequin. I had not attended any sort of training so I was taken aback when a mannequin started responding to my questions.
During our time in Uk, we were smitten by the country, the beautiful landscapes , the polite and seemingly jolly good fellows, (more about the British politeness in later articles), I must say ,we were truly blown away, in that 1st visit.

I cleared PLAB 2, got my GMC registration, applied for jobs, had Skype interviews and very easily secured my 1st job in Wales, Uk. Do note, by this stage my pocket was lighter by just a few more lakhs but all for a brighter future ain 't it mates !
I worked as a LAS Specialty Registrar in General medicine for about 8 months, during which time I studied for yet another exam ! The MSRA (Multi- speciality Recruitment Assessment), which had 2 parts, one MCQ and a second face to face part called a selection centre, since Covid this part of the exam does not exist.
*MSRA is a Mult speciality recruitment exam, and I was encouraged by many to apply for some other specialities. Also, while working as a medical registrar, there were consultants, mostly Indian consultants, who gave me advice about this being a second chance to choose another specialty, 'Go for IMT (Internal Medicine Training) and then aim to get into specialty training and become a specialist', nothing wavered my love for family medicine. I stuck to my goal of becoming a GP with yet another degree. *
After the nth exam I finally got into GP training in Uk and for this, I moved to 'Wee Bonnie Scotland' in February 2020.

Why the Move Was Worth It
For a change, The fun of living in a different country, Going to college in a foreign university, Better education, More money !!!, Doggie. The last 2 are still pending and perhaps I am never going to get a dog. She may in future. She has achieved the rest on her list.
As for my husband and me, it was the opportunity to work less but earn reasonably well, living a good life now and not waiting for retirement to do things we like doing. It was never about money and in my opinion, nobody should base their lives only on how much they earn.

I have learnt that life is truly richer when you get to do things you love to do on a regular basis, without having to stress yourself about everyday life. 'Living life to the fullest with those you love' that's my dream life and I think I have achieved this.
So, until next time, I wish you all luck in achieving the dream life! I'll be back with details of GP training in Uk and life in Scotland !
Doctor in the Spotlight
Service Without Borders: From Uniform to Family Medicine
Service Without Borders: A Physician's journey from Uniform to Family Medicine
Col (Dr) Mohan Kubendra, Consultant Family Medicine & Diabetologist, Founding Director Spandana Health Care, Bengaluru, National President, Academy of Family Physicians of India (AFPI)
I have always believed that the success of an individual should be judged not by where one finally reaches, but by where one begins. Perhaps that belief comes from my own background. I did not start life with privilege or legacy, but with modest means, strong values, and parents who led by example rather than instruction. Looking back, I realise that every doctor, every human being has a story worth telling. Not because it is extraordinary, but because it may resonate with someone else standing at a crossroads. This is my story.
Life in Uniform: Learning Beyond Medicine
After completing my medical graduation, life presented me with a familiar dilemma faced by many young doctors from middle class families- idealism versus responsibility. With my father approaching retirement and my brothers still finding their footing, financial security became an immediate necessity. While postgraduate education was an aspiration, it was not a practical option at that stage. Yet, one passion remained non-negotiable: the desire to serve the nation in uniform. That conviction led me to join the Indian Armed Forces as a commissioned medical officer, a decision that would define the next 22 years of my life.
Armed Forces gave me experiences that no textbook could. I treated young soldiers anxious before deployment, tended to officers far from their families, and worked through emergencies, insurgencies, in difficult terrains, where teamwork mattered more than hierarchy. Medicine in uniform is not just about treating illness; it is about readiness, resilience, and responsibility to the individual soldier and to the system as a whole. Those years instilled in me a profound respect for structured systems, discipline, and service above self. Later, postgraduate training in Aerospace Medicine and Hospital Administration introduced me to the larger system- how policy, planning, and logistics affect patient care. Yet, even as I grew professionally, a quiet thought would occasionally surface during patient interactions: What happens to people once they leave the system? Who looks after them in the long run?


The First Pull Towards Family Medicine
That question became clearer while I was on foreign deputation during my interactions with doctors from Bhutan who had trained in Family Medicine. I remember listening to one of them speak about caring for three generations of the same family, knowing their illnesses, anxieties, and social contexts intimately. It struck me then that this was the kind of doctor I instinctively trusted and perhaps wanted to become.
Deciding to pursue DNB Family Medicine while still in uniform was not easy. Colleagues wondered why I would take such a step when my career was stable and predictable. I wondered too, especially on days when logic seemed louder than instinct. But conviction has a way of persisting. So, I reported for my DNB residency at a 650- bedded Army Base Hospital, hopeful and curious.
Residency: When Reality Teaches You
Reality, however, was sobering. We were three Family Medicine residents, supervised by a sincere Internal Medicine consultant who openly admitted that he wasn't quite sure what Family Medicine training was supposed to look like. There were no structured objectives, no faculty from the specialty, and no professional association like AFPI to turn to. Administrative duties as officers in uniform continued alongside clinical work. I still remember standing in the ICU one night after a particularly long shift, wondering if I had made a serious error in judgment. This was not the residency experience I had imagined. But something interesting happened over time. We were posted wherever there were gaps—casualty, wards, speciality OPDs, ICU. We learnt to handle emergencies, coordinate care, and make decisions across specialties. Slowly, almost without realizing it, we were learning exactly what Family Medicine demands: breadth, adaptability, and confidence in uncertainty. With no formal structure, we created our own.
As the final examination approached, the atmosphere was heavy with doubt. Two senior batches before us had failed. No Armed Forces doctor had cleared DNB Family Medicine until then. One evening, during a discussion among ourselves, someone said, "Let's just give it one honest attempt. We really have nothing to lose." That moment changed everything. Accepting the possibility of failure lifted a weight we didn't realize we were carrying. There after we prepared with quiet determination and an unspoken sense of solidarity. When four of us cleared DNB Family Medicine from Armed Forces, it felt surreal. More than personal success, it felt like validation- that perseverance still mattered, even within imperfect systems. That phase taught me one of my most enduring lessons: 'learning is not always delivered neatly; sometimes it must be assembled patiently'.

From Military Service to Community Care: A Physician's Transition
Taking voluntary retirement from the Armed Forces was one of the most difficult decisions of my life. The uniform had given me identity, structure, and purpose. Letting go of it was not easy. I remember my first few months after retirement- walking into civilian clinics without rank insignia, without the familiar system around me. It was unsettling. But it was also liberating. I knew by then that my heart lay in community- based practice, in seeing patients over time, understanding family dynamics, and being present not just during illness but through life events.
Returning to Bangalore, I started two day- care primary care clinics right away in suburban Bengaluru. As my practice matured, I consciously chose to keep it community- oriented rather than hospital- centric. The clinic became a place where follow- ups were unhurried, referrals were thoughtfully coordinated, and unnecessary investigations were discouraged. Over time, families began returning, not just for treatment, but for advice, reassurance, and continuity. That trust reaffirmed everything I believed about Family Medicine.
The COVID- 19 pandemic further reinforced the value of this approach. During that uncertain period, the clinic transformed into a point of reassurance. Patients called not just for prescriptions, but to ask whether their symptoms were serious, whether it was safe to step out, or simply to hear a familiar voice. Teleconsultations blurred the boundaries between clinic and home, reminding me that Family Medicine adapts instinctively to changing circumstances.
Reflections on AFPI and Leadership
My association with AFPI has had a profound influence on my practice. From senior colleagues, I learnt the finer nuances of ethical, patient- centred family practice, shaped by experience and wisdom. From my younger colleagues, I learnt the importance of staying updated, embracing change, and continually striving for excellence. Together, these interactions have kept my practice relevant, reflective, and grounded. I was fortunate to be involved in building AFPI Karnataka from its inception, a journey that truly tested and refined my leadership skills. It taught me how to listen, build consensus, mentor young colleagues, and translate shared vision into meaningful action.

It has now been nearly 13 years since I retired from the Armed Forces. While I miss life in uniform, I can say without hesitation that my post- retirement years have been the most professionally fulfilling.
Reflections on the Future
Family Medicine in India faces undeniable challenges. Medical education remains largely tertiary- care focused. Young doctors rarely see strong role models in community- based practice. Career pathways remain unclear, especially within government systems. Many would opine Family medicine now is a bit of a dying practice. Yet, I remain hopeful. India is still a society that values personal doctors. Gated communities, urban neighbourhoods, and assisted living facilities offer enormous opportunities for sustainable family practice. What we need are model clinics and mentorship structures that allow young doctors to see what is possible.
With Artificial Intelligence(AI) disrupting many medical specialties and transforming healthcare, one thing is becoming clearer to me: technology may assist diagnosis and medical procedures, but it cannot replace human touch and empathy that defined Family physicians. Patients today are overwhelmed with information. What they seek is a doctor who listens, contextualizes, and cares. That role belongs naturally to the Family Physician and he remains indispensable. I firmly believe that as healthcare evolves, it will slowly gravitate back towards qualified Family Medicine specialists.
In Gratitude
I remain deeply grateful to Dr Raman Kumar for placing his trust in me, for entrusting me with leadership responsibilities within AFPI, and for allowing me to step into his role as National President. I am equally thankful to my colleagues who have walked this journey alongside me. I owe special gratitude to my mentor Dr BC Rao, from whom I learnt not only professional wisdom but also how to transition gracefully from life in uniform to civilian practice.

From service in uniform to universal service, the journey has been deeply meaningful. If there is one message, I would like young doctors to take from my story, it is this: 'Family Medicine is not a compromise. It is a commitment to people, to communities, and to the human side of healing. It is a calling and the community deserves it as much as you deserve the most gratifying profession'. Jai Hind !!
Fun Zone
What's the Next Step? Brain teasers
What's the Next Step? (Clinical Reasoning Cases)
Choose the SINGLE best next step
Case 1
A 45- year- old man visits for an annual check- up. He has no known medical illnesses and feels well.
Findings: BP: 146/92 mmHg (two readings in clinic), BMI: 28 kg/m², Fasting glucose: 98 mg/dL, No target- organ damage.
Next step?
A. Start antihypertensive medication immediately
B. Order ambulatory blood pressure monitoring
C. Reassure and review after 1 year
D. Refer to cardiologist
Answer: B. Order ambulatory blood pressure monitoring
Case 2
A 38- year- old woman presents with low back pain for 3 weeks. Pain is dull, localized, worse at the end of the day.
Findings: No trauma history, No fever, weight loss, or night pain, Neurological examination normal.
Next step?
A. MRI spine
B. X-ray lumbosacral spine
C. Reassure, advise activity modification and analgesia
D. Refer to orthopaedic surgeon
Answer: C. Reassure, advise activity modification and analgesia
Case 3
A 60- year- old woman comes for routine follow- up. She has hypertension, well controlled on one medication.
Findings: BP: 128/76 mmHg, Pulse: 72/min, She reports occasional light-headedness on standing, No falls, no chest pain, Electrolytes normal.
Next step?
A. Add another antihypertensive to reach lower targets
B. Stop antihypertensive medication completely
C. Check postural blood pressure and review dose timing
D. Refer to cardiology
Answer: C. Check postural blood pressure and review dose timing
Case 4
A 34- year- old woman presents with recurrent abdominal bloating and loose stools for 6 months. Symptoms worsen during stress and improve on holidays.
Findings: Normal appetite, No weight loss, No blood in stools, Normal haemoglobin and basic labs, Abdomen soft, non-tender.
Next step?
A. Colonoscopy
B. CT abdomen
C. Diagnose irritable bowel syndrome and initiate dietary modification
D. Start empirical antibiotics
Answer: C. Diagnose irritable bowel syndrome and initiate dietary modification
Medical word puzzles for fun learning
Anagram Diagnosis
1. LIP ON A RUST
Clinical clue: Young woman with recurrent miscarriages and unexplained thrombosis.
Answer: ANTIPHOSPHOLIPID SYNDROME
2. SALT RAIN
Clinical clue: Sudden onset focal neurological deficit that completely resolves within 24 hours.
Answer: TRANSIENT ISCHEMIC ATTACK
3. PAIN CURE HIT
Clinical clue: Severe epigastric pain radiating to the back, worsened after alcohol intake.
Answer: ACUTE PANCREATITIS
4. HOT MEAL
Clinical clue: Painful swelling following trauma or anticoagulant use.
Answer: HAEMATOMA
5. CARPET SIN
Clinical clue: Acute hot, swollen joint with fever and restricted movement.
Answer: SEPTIC ARTHRITIS
Word Search Puzzle
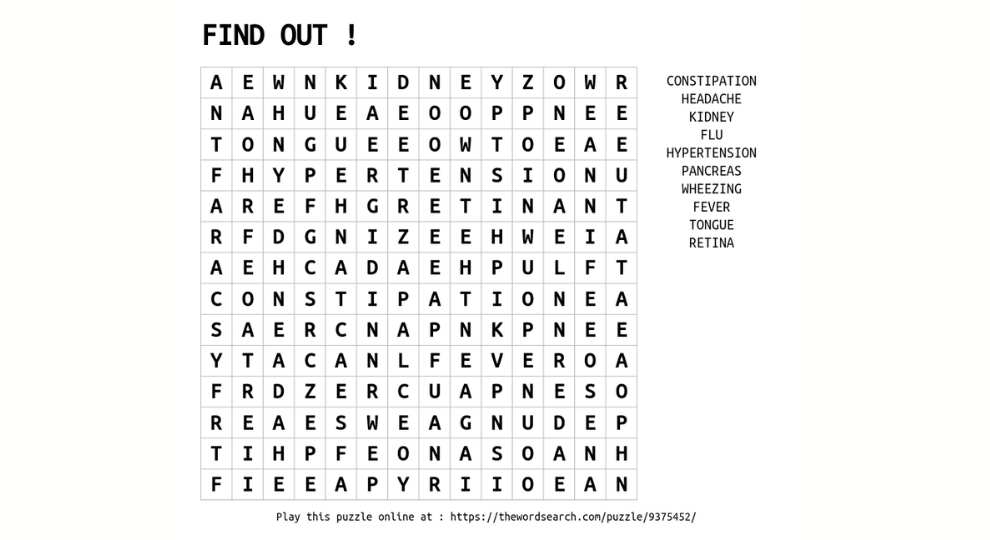
Find medical terms in the grid
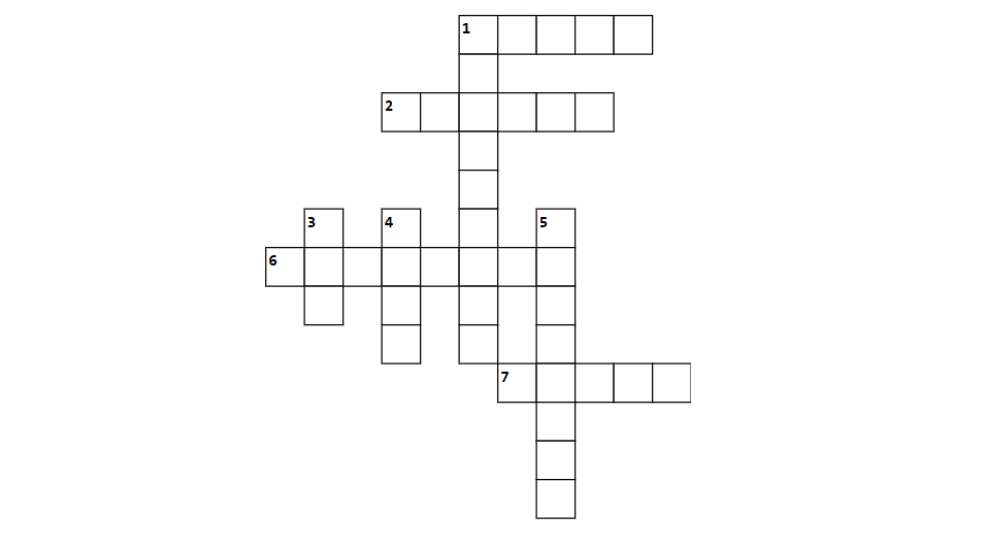
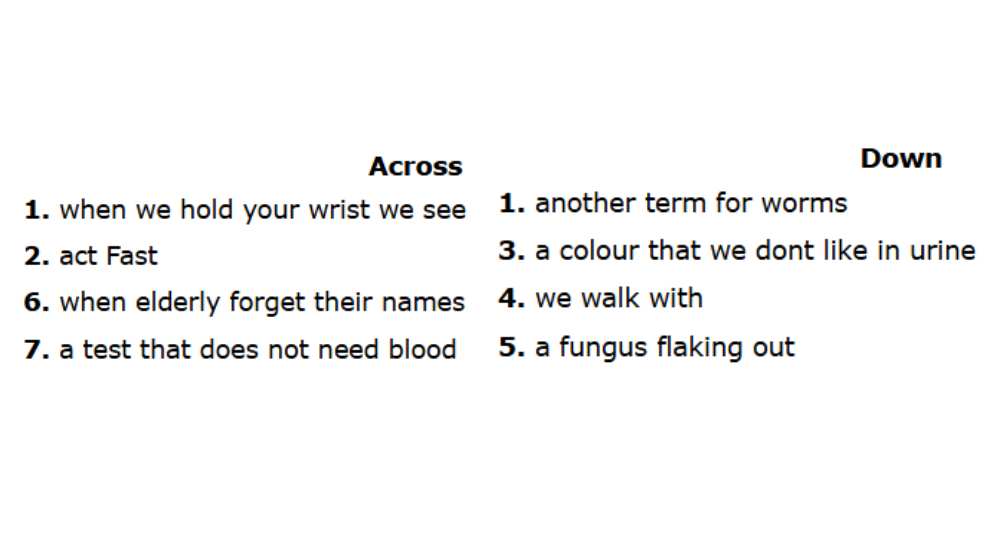
Crossword Puzzle
Medical Jokes
Doctor-Patient Interaction:
My doctor told me to watch my drinking—now I drink in front of a mirror!
The Walking Problem:
Doctor: Walk for 30 minutes every evening.
Patient: I can't do evenings, doctor.
Doctor: Why not?
Patient: That's when my TV serial is on. Tomorrow the heroine has a job interview... it's very stressful.
Sleep Advice:
Doctor: You need at least 8 hours of sleep.
Patient: I sleep 10 hours, doctor!
Doctor: That's great. At night?
Patient: 6 at night... 4 in office meetings
Detective Doctors - Case Discussions
Case: The Young Woman with Fatigue
A 32- year- old woman, recently married (6 months), presents with progressive shortness of breath, easy fatigability, and palpitations for the past 3 months.
She says, "Doctor, earlier I could climb two floors easily. Now even one flight makes my heart race."
She also reports: Occasional dizziness, Reduced exercise tolerance, No cough, wheeze, or chest pain, No fever or weight loss. No past history of heart disease. No smoking.
On Examination: Pulse: 96/min, regular, BP: 110/70 mmHg, SpO2: 98% at rest, Pallor: Present, JVP: Normal, Cardiovascular: Flow murmur present, Respiratory system: Clear, No pedal oedema.
Investigations (done outside): Hb: 8.6 g/dL, MCV: 68 fL, Serum ferritin: 6 ng/mL, TSH: 2.4 mIU/L, ECG: Sinus tachycardia, Chest X-ray: Normal.
On gentle probing, she mentions: "My periods have always been heavy... but I thought that's normal."
What's the MOST LIKELY DIAGNOSIS?
A. Dilated cardiomyopathy
B. Panic disorder
C. Iron deficiency anaemia causing high-output state
D. Pulmonary embolism
Answer: C. Iron deficiency anaemia causing high-output state
Brain Teaser Corner - Answer Key
Crossword Answers:
ACROSS: 2. URIC | 5. PLATELET | 9. HBA1C | 10. FIVE | 12. MOUTH | 13. APPLE | 14. VACCINE
DOWN: 1. ORS | 2. RETINA | 3. VACCINE | 4. TSH | 5. CALCIUM | 6. BCG | 7. METFORMIN
Detective Case 1 Answer
Answer: B. Secondary hypothyroidism (pituitary origin)
Despite a "normal" TSH, the low Free T3 with low- normal Free T4 and classic hypothyroid signs (bradycardia, delayed reflexes, dry skin) point to central hypothyroidism, where TSH is inappropriately normal and misleading.