📑 CONTENTS
👥 Leadership & Editorial

Dr Sowmya B Ramesh
President Karnataka
Warm greetings from the AFPI Karnataka Chapter.
This quarter has been quite productive, with the successful conduct of a conference in collaboration with BAPTIST HOSPITAL. Following that, we organized focused updates on topics such as herpes vaccines, pneumococcal vaccines, which are highly relevant to our current vaccination practices.
We are delighted to announce an upcoming full-fledged offsite meeting in Mysore on June 7th. The program details have already been shared, and we encourage all members to ensure their availability and actively participate to make the event engaging and impactful.
We are also excited to share plans for a rural conference in Atheni, North Karnataka, scheduled for November. In addition, we have several webinars and in-person events lined up, covering topics such as dog bite management, artificial intelligence in healthcare, and a rheumatology workshop.
We look forward to your enthusiastic participation and valuable contributions in all these initiatives.
Warm regards
Dr. Sowmya B Ramesh , President, AFPI Karnataka

Dr Hemavathi, Secretary AFPI Karnataka
Dear Members,
Greetings from AFPI Karnataka.
As part of our continued commitment to academic excellence and professional development, we are pleased to share that we have planned regular academic activities on a monthly basis for the upcoming quarter.
The sessions will cover a range of relevant and engaging topics, including Sarcopenia, Artificial Intelligence in Healthcare, and Management of Dog Bites, among others. These sessions are designed to enhance our clinical practice and keep us updated with evolving trends in family medicine.
In addition, we are organizing a Half-Day CME in Mysore, which will provide an excellent platform for knowledge exchange and interaction. We are also excited to announce the upcoming Rural State Conference in North Karnataka, focusing on addressing healthcare challenges and innovations in rural settings.
We strongly encourage all members to actively participate in these academic initiatives. Your involvement will not only enrich your own practice but also strengthen our collective mission of advancing family medicine across the state.
We look forward to your enthusiastic participation and continued support.
Warm regards,
Dr Hemavathi,
Secretary AFPI Karnataka

EDITOR'S DESK
Medicine is no longer a fixed rulebook---it is a living, evolving science.
What we learned yesterday may not fully serve the patient of today.
Guidelines remain our compass, but not our cage.
True clinical wisdom lies in knowing when to follow---and when to thoughtfully question.
As new evidence emerges, so must our thinking adapt with humility.
Innovation often begins where rigid adherence ends.
Yet, progress demands responsibility, not reckless deviation.
We must stay curious, continuously learning, unlearning, and relearning.
Our patients deserve care that reflects both science and insight.
In these changing times, the best doctors are those who evolve without losing their core.
Dr. Amina Kausar Shah
doctoraminaa@gmail.com
🧠 Clinical Wisdom & Practice Pearls

PEARLS OF DR. BADAKERE RAO
Do Not Die Before I Die
As I get old and conscious that not many years of reasonably competent professional life remains, I often think about what happens to my patients after my inevitable demise. These men and women have been my patients, often running to several generations.
The relationship and bond built over several decades is so subtle yet so strong that it is difficult to describe. Occasionally when this subject of inevitable mortality comes up during our talk, I tell them, "It is time you find another family doctor" This invariably leads to comments like, we will see when the time comes or "doc, you please suggest someone you think best" and the like. But what really exemplifies this bond is when this 70-year-old, Mrs. Yasmin told me the other day, "for heaven's sake, doc, don't go and die before I die"
Lets Get a Pearl out of Dr Rao now - A case of recurrent Bell's Palsy !
Does Bell's palsy have a genetic predisposition?
Both recurrence and genetic predisposition appearing in the same patient is uncommon.
Mr Sivasailam, A 60-year-old retired IT professional came with complaints of facial weakness, dribbling of saliva from one half of his mouth in the month of May 2017 which clinically was Bell's palsy. He recovered well with a course of prednisolone and Physiotherapy in 3 months' time. He reported on 2nd November 2035 with similar complaints, this time on the left side. He gave a history of his father suffering from similar symptoms and his UK based son having this in the month of July 2025.
Bell's Palsy is generally a common condition, occurring in about 1 in 60 people over a lifetime, its occurrence across three generations of males in a single family and its recurrence in the same person are uncommon but well-documented phenomena in medical literature, suggesting a genetic predisposition in these specific cases.
Recurrence in the Same Person
• Overall Rate: Recurrence of Bell's Palsy is relatively rare in the general population, reported to be in the range of 2.6% to 15.2% of patients who have had a primary episode. A commonly cited average is about 7-10%.
• Increased Risk with Family History: The likelihood of recurrence is greater in individuals who have a positive family history of the condition.
• Multiple Episodes: While most people only have one or two episodes, some rare cases have reported as many as five or six episodes in the same individual.
• Recurrence Pattern: Recurrences can affect the same side of the face (ipsilateral) or the opposite side (contralateral).
Familial Occurrence (Across Generations)
• Prevalence: A positive family history is found in approximately 4% to 14% of all Bell's Palsy cases. In some studies, this figure can range up to 28.6%.
• Inheritance Pattern: Familial Bell's Palsy often follows an autosomal dominant inheritance pattern with low or variable penetrance, meaning that not everyone who inherits the genetic predisposition will develop the condition. In some rare case studies, high or complete penetrance has been noted.
• Male-Only Pattern: While the condition generally affects males and females equally, a presentation specifically in males across three generations would be considered a rare, but possible, manifestation of this genetic predisposition. Medical literature includes case series describing familial occurrences over multiple generations, but a strictly male-only lineage across generations would be an unusual and specific presentation.
• Cause: No specific gene has been definitively identified as the sole cause of Bell's Palsy; the prevailing theories suggest a combination of genetic susceptibility (possibly related to anatomical narrowing of the facial canal or immune response genes) and environmental triggers like viral infections.
In summary, having a case of Bell's Palsy run in a family for three generations and recur in the same individual points towards a genetic predisposition, which is a recognized, albeit uncommon, form of the condition.
The occurrence of Bell's palsy in three generations of the same family and with recurrence in the same person is considered rare but well-documented in medical literature. While most cases are sporadic (not inherited), a genetic predisposition is a known risk factor, and familial cases have a higher likelihood of recurrence.
Dr. B.C.Rao
📚 Academic Update: Tuberculosis Diagnosis & Management

AN UPDATE ON TUBERCULOSIS : DIAGNOSIS AND MANAGEMENT
Dr. S Subramanyam , Family Physician
Signs and symptoms of TB
Latent TB
Infected but no signs and symptoms. About 40% of Indian and 25% of global population are having latent TB out of which only about 5% may develop active TB under various immunosuppressive conditions.
TB can affect any system in the body from head to toe except hair and nail and the symptoms depend on the system affected. Common symptoms are fever, cough, loss of appetite and weight but symptoms can be acute or chronic, mild, moderate, or severe.
Whenever there is a diagnostic challenge, after ruling out all the other possibilities Tuberculosis must be considered and sometimes empirical treatment may have to be given for diagnostic / therapeutic purpose.
Latent TB SHOULD be treated in high-risk groups, HIV and immunosuppressed
Classification :
Is now simplified as DSTB ( Drug Sensitive TB) and DRTB ( Drug Resistant TB).
Diagnosis
Tissue diagnosis is a must from the suspected material. Sputum / biopsy material to be subjected for histopathology, ZN stain and CB-NAAT ( GeneXpert)
CB-NAAT picks up only MTB even in very low concentration and gives information whether there is Rifampicin resistance.
Those who are Rifampicin resistant are invariably resistant to INH also, and fall in to the category of DRTB. Rifampicin resistance is a strong surrogate marker for MDR-TB and often associated with INH resistance
It is mandatory to clarify DSTB or DRTB before starting treatment because DRTB is on the rise, is very dangerous, difficult to treat and often fatal.
Culture and sensitivity : If CB-NAAT confirms Rifampicin resistance, material should be sent for Liquid culture ( Bactec ) we get results in about 2 to 4 weeks.
LPA ( Line Probe Assay ) : LPA is a rapid technique based on polymerase chain reaction (PCR) that is used to detect Mycobacterium tuberculosis (MTB) complex as well as drug sensitivity to rifampicin and isoniazid (INH)
Treatment of TB
Is simplified only two categories DSTB or DRTB. DSTB treatment is same for TB anywhere and any severity.
Drugs used are HREZ ( INH, Rifampicin, Pyrazinamide and Ethambutol) for first two months ( Intensive phase) and HRE for 4 months ( continuation phase). Duration may be extended in special cases like CNS, Bone and joint TB, delayed response, and the like.
Dosing also made easy with FDC ( Fixed Drug Combination) one tablet for 15 kg body weight.
Supportive treatment
Adequate nutrition and management of side effects is important..
Any Multivitamin containing Pyridoxine 10 mg is sufficient, it is observed that Pyridoxine is being prescribed in the dose of 40 mg without any indication.
DRTB ( Drug Resistant TB)
MDR,XDR and all resistant TB come under DRTB. Treatment of DRTB is based on the culture and sensitivity pattern.
Drugs used are toxic with lot of side effects, preferably treated by an expert in an institution under careful monitoring of the side effects.
The introduction of Bedaquiline has revolutionized the management of DRTB.
New regimens, do not have injectable and duration of 12 months, efforts are on to make it 6 to 9 months.
Primary care physicians are advised to manage DRTB in association with an expert from / in an institution.
Side effects of ATT
Common side effects are nausea, vomiting, burning stomach, bowel disturbance, giddiness, burning feet, skin rashes.
Most important and dangerous side effect is hepatotoxicity, if not attended in time can be fatal. Liver enzymes elevated up to 3 times with symptoms and up to 5 times without symptoms can be accepted and treatment continued.
Above that, treatment should be stopped and can be reintroduced after liver enzymes return to normal
Interestingly, most do not develop hepatotoxicity second time, if they do, we have to revise the combination. Routine high-dose pyridoxine is unnecessary unless risk factors (diabetes, alcohol use, pregnancy, malnutrition) are present.
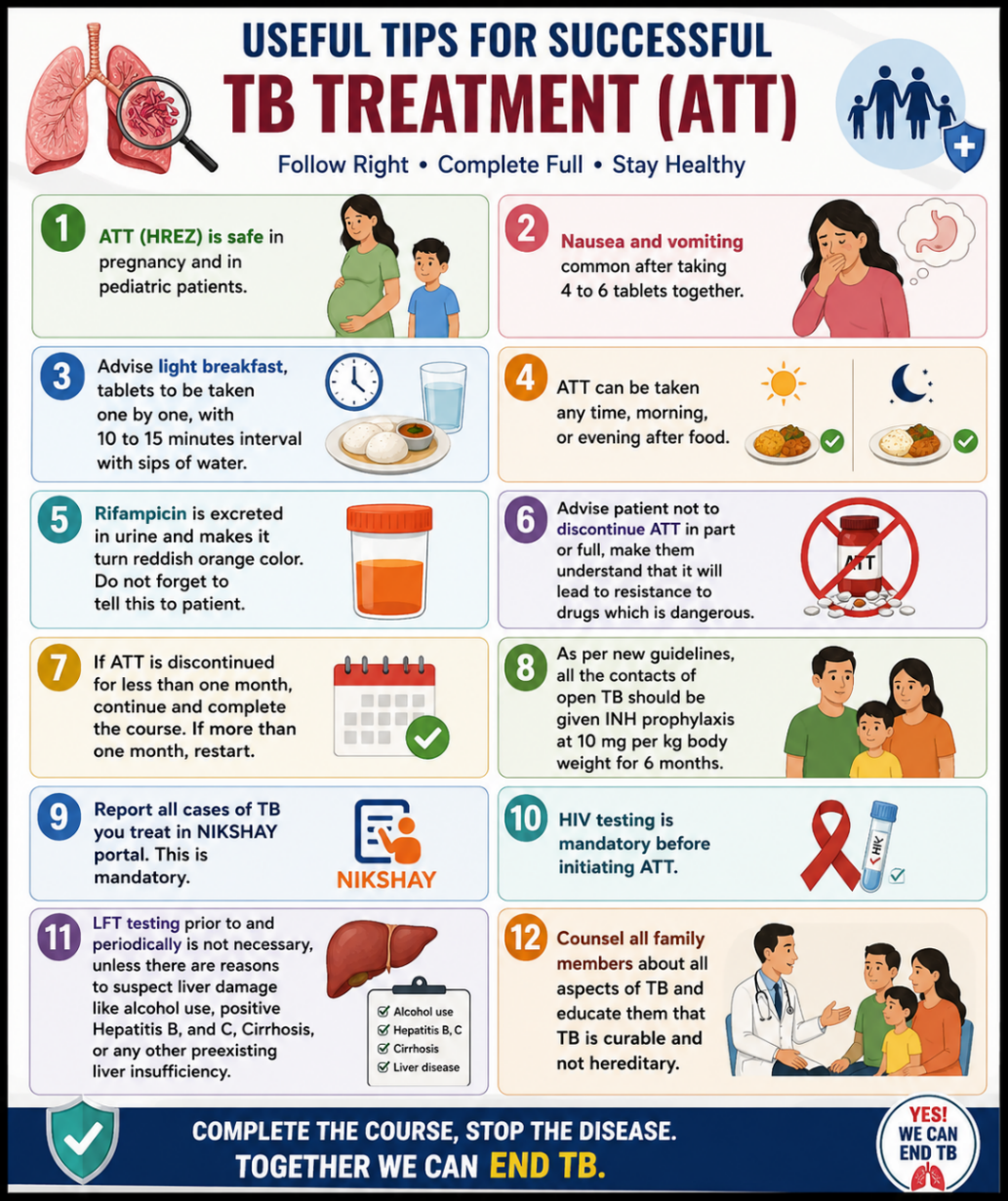
Some useful tips
First line ATT HREZ is safe in pregnancy and in pediatric patients
Nausea and vomiting common after taking 4 to 6 tablets together.
Advise light breakfast, tablets to be taken one by one, with 10 to 15 minutes interval with sips of water. ATT can be taken any time, morning, or evening after food.
Rifampicin is excreted in urine and makes it turn reddish orange color. Do not forget to Inform the patient. Advise patient not to discontinue ATT in part or full, make them understand that it will lead to resistance to drugs which is dangerous.
If ATT is discontinued for less than one month, continue and complete the course, If more than one month, restart.
As per new guide lines, all the contacts of open TB should be given INH prophylaxis at 10 mg per kg body weight for 6 months.
Report all cases of TB you treat in NIKSHAY portal. This is mandatory.
HIV testing is mandatory before initiating ATT.
LFT testing prior to and periodically is not necessary, unless there are reasons to suspect liver damage like alcohol use, positive Hepatitis B, and C, Cirrhosis, or any other preexisting liver insufficiency.
Counsel all family members about all aspects of TB and educate them that TB is curable and not hereditary.
There is an excellent system under NTEP ( National Tuberculosis Elimination Program) for diagnosis and treatment, totally free of cost, make best use of it.
Family Physician is the first contact for most health- related issues, he has the advantage of early detection, management, prevention of spread, prevention of DRTB and he is the key in reaching the goal. Until family physicians are updated and committed in the TB elimination program, this program cannot be successful. It is the responsibility of the family physician to diagnose and treat all forms of TB unless the patient needs surgical intervention or hospitalization.
Guidelines keep changing, keep in touch with NTEP website and keep pace with the latest guidelines.
Dr S Subramanyam
Family Physician
M : 9845029954
E- mail : subbusarof@yahoo.com
📈 Clinical Updates
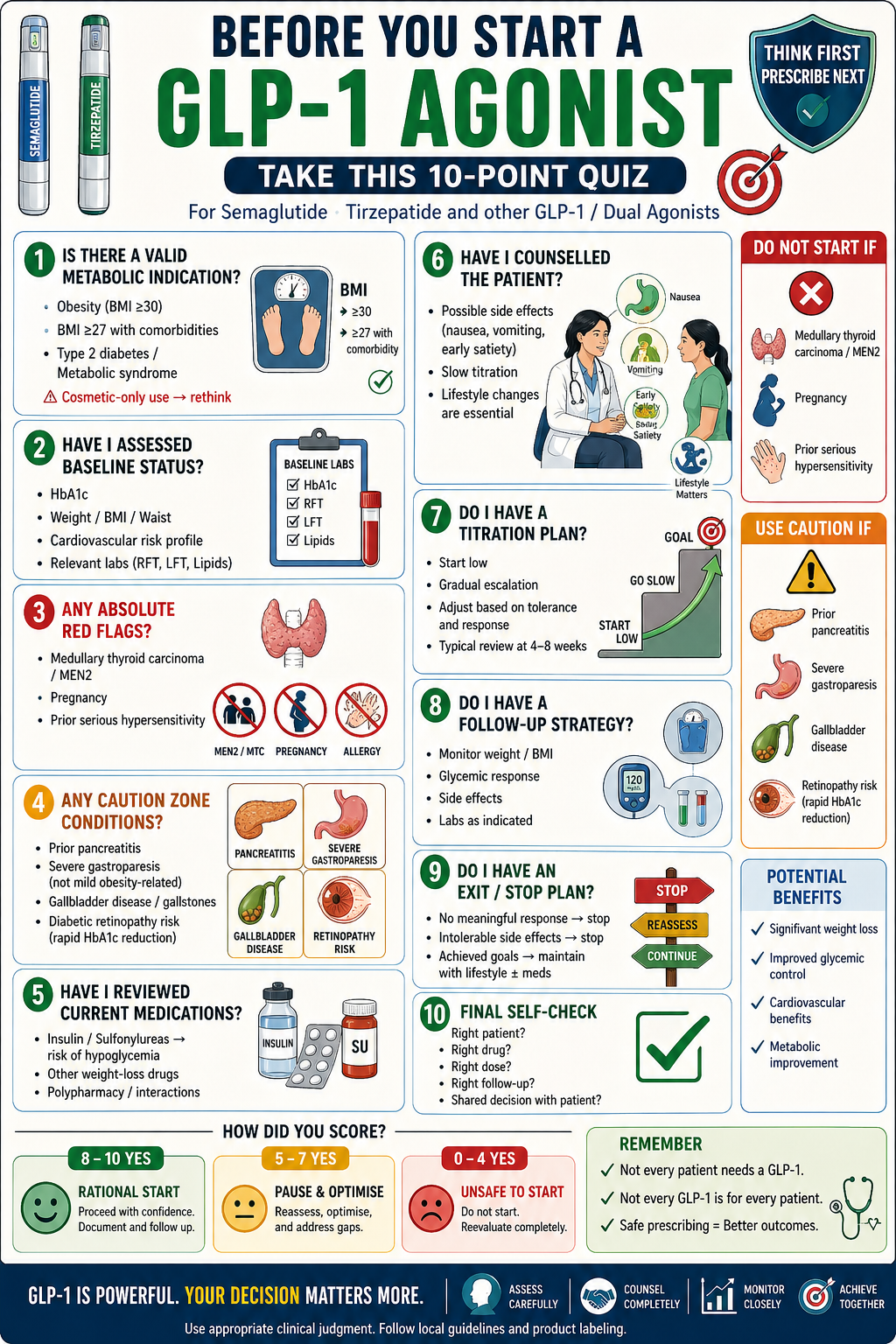
Are You GLP-1 Agonist Prescribing Ready?
Dr. Amina Kausar Shah
Things Every Physician Must Know
1. Shift in role: GLP-1 RAs are now obesity-first drugs, not just antidiabetics.
2. Disease model changed: Obesity is treated as a chronic relapsing endocrine disease, not lifestyle failure.
3. Best-in-class currently: Tirzepatide > Semaglutide for both HbA1c and weight loss.
4. Expected weight loss: Semaglutide ≈ 12--15%; Tirzepatide ≈ 20--22%.
5. Next-gen drugs incoming: Triple agonists (e.g., retatrutide) may achieve 25%+ weight loss (near bariatric outcomes).
6. Oral revolution: Oral GLP-1s (like Oral Semaglutide) are expanding access and compliance.
7. Cardiovascular benefit: ~20% reduction in major adverse cardiovascular events (MACE).
8. Renal protection: Slows CKD progression---now entering nephrology practice.
9. Not just metabolic: Emerging roles in fatty liver, PCOS, and possibly neurodegeneration.
10. CNS effects: Reduce food reward, cravings, and possibly addictive behaviours (alcohol, nicotine).
11. Common side effects: Nausea, vomiting, constipation---dose titration is key.
12. Newer red flags: Watch for -Vision changes (optic neuropathy- Evidence is weak / emerging), Mood changes / depression, Fatigue.
13. Weight regain is common: Stopping therapy → rapid regain (this is lifelong therapy for many).
14. Adherence problem: Up to ~50% discontinue within 1 year (cost + side effects).
15. Big clinical shift: GLP-1s are now multi-system disease-modifying drugs, not just glucose-lowering agents.

Higher Generation is Not Better: Choosing the Right Cephalosporin in Primary Care
Dr. Krithika Ganesh
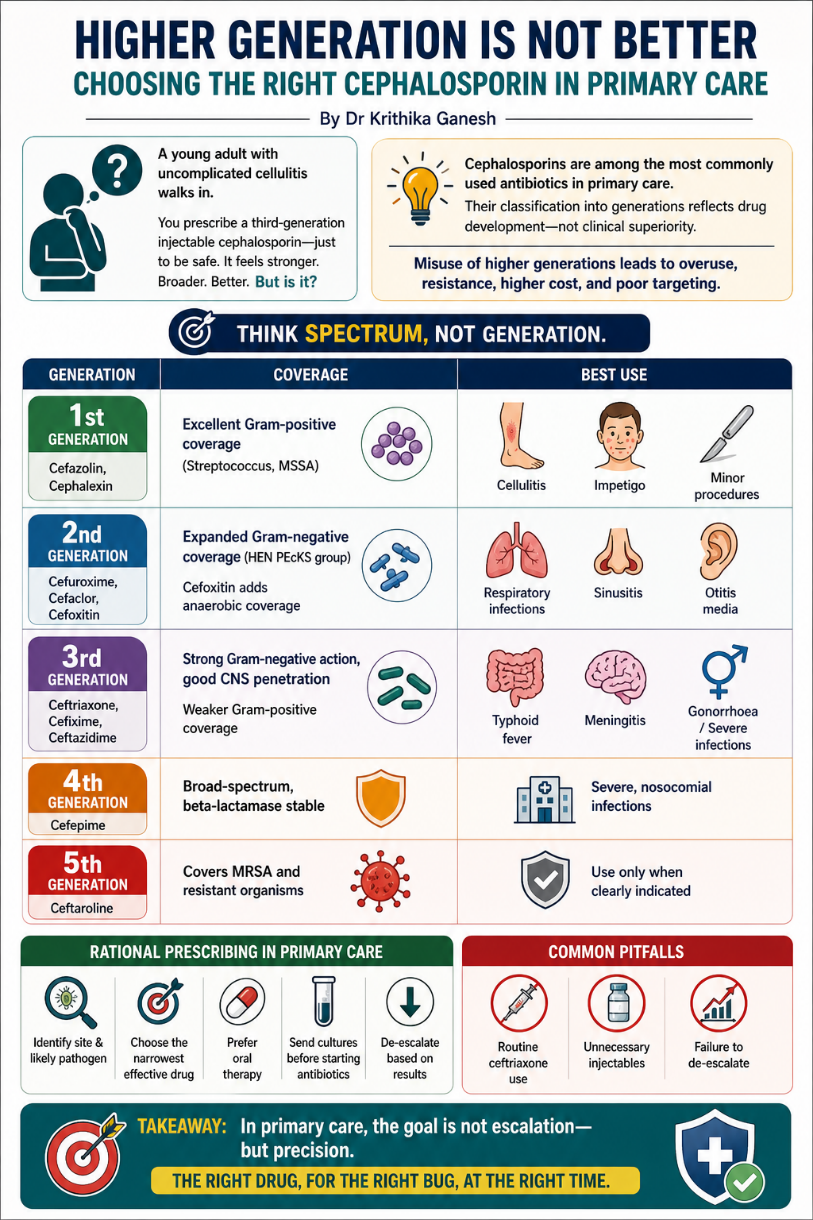
A young adult with uncomplicated cellulitis walks in. You prescribe a third-generation injectable cephalosporin---just to be safe. It feels stronger. Broader. Better. But is it?
Cephalosporins are among the most commonly used antibiotics in primary care. Their classification into generations reflects drug development---not clinical superiority. Misinterpreting this leads to overuse of higher generations, poorer targeting, rising resistance, and unnecessary cost.
Think spectrum, not generation.
First-generation (cefazolin, cephalexin): Excellent Gram-positive coverage (Streptococcus, MSSA). Best for cellulitis, impetigo, folliculitis, minor procedures.
Second-generation (cefuroxime, cefaclor, cefoxitin): Expanded Gram-negative coverage (HEN PEcKS group). Useful in respiratory infections, sinusitis, otitis media. Cefoxitin adds anaerobic coverage.
Third-generation (ceftriaxone, cefixime, ceftazidime): Strong Gram-negative action, good CNS penetration. Weaker Gram-positive coverage---avoid for typical SSTIs. Use in typhoid, meningitis, gonorrhoea, severe infections.
Fourth-generation (cefepime): Broad-spectrum, beta-lactamase stable. Reserved for severe, nosocomial infections.
Fifth-generation (ceftaroline): Covers MRSA and resistant organisms. Use only when clearly indicated.
Rational prescribing in primary care:
-Identify site and likely pathogen
-Choose the narrowest effective drug
-Prefer oral therapy
-Send cultures before starting antibiotics
-De-escalate based on results
Common pitfalls:
- Routine ceftriaxone use
- Unnecessary Injectables
- Failure to de-escalate
Takeaway- In primary care, the goal is not escalation---but precision.
💬 Reflections, Technology & Career Pathways

Between Consultations
By Dr. Archana Prabhakar
On Being "Ready": The Quiet Work of Showing Up!
Entering medical school felt extraordinary---and terrifying. Beneath the pride lived quieter questions: Am I good enough? Will I manage? What if I fail?
These doubts didn't fade---they stayed. Through first year confusion, final year expectations, and into practice.
Looking back, one truth stands out: readiness never comes before responsibility.
Not before exams.
Not before rural postings.
Not before opening a clinic.
And yet, we show up.
Family medicine in India demands this daily. Patients arrive not with diagnoses, but with layered realities---social, emotional, financial. In ten minutes, we must listen beyond symptoms.
"Swalpa weakness" may mean anaemia---or burnout.
Here, readiness isn't knowing everything.
It is staying present despite uncertainty.
Evidence supports what we see daily---empathy improves outcomes, adherence, and trust. Yet training often erodes it. Family medicine resists this by valuing relationships.
But empathy has a cost. Compassion fatigue is real. Sustainable care requires self-awareness, reflection, and boundaries.
Rural postings teach this best---where medicine strips down to listening, observing, and deciding when not to intervene.
Choosing family medicine means choosing continuity over certainty. Meaning over metrics.
Readiness, then, is not a milestone.
It is built quietly---through conversations, mistakes, reflection, and return.
Perhaps the question is not when we are ready---
but how we continue to show up, even when we are not !!

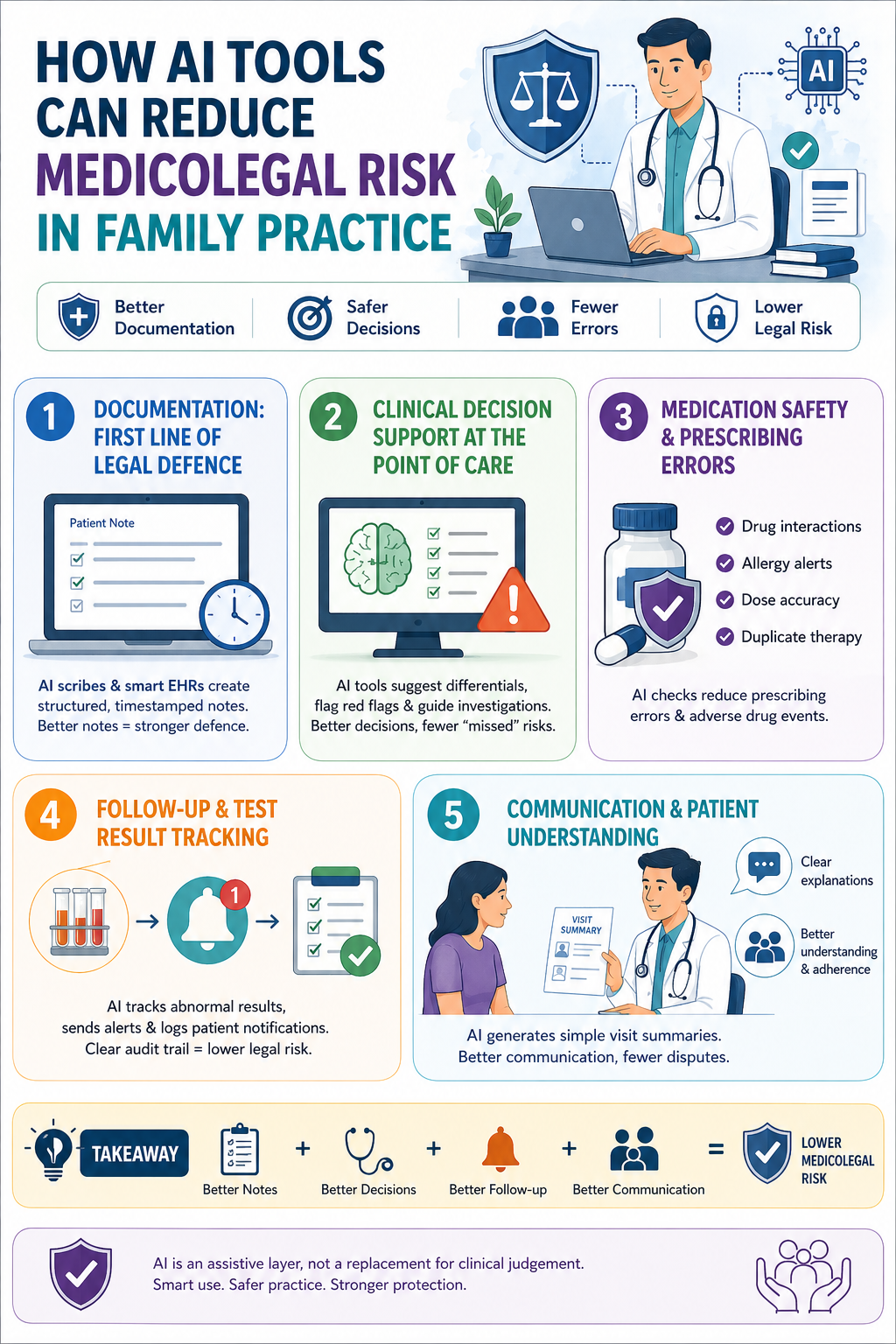
How AI Tools Can Reduce Medico-Legal Risk in Family Practice
Dr. Syed Mubarak
As family physicians, we work in a high-volume, high-trust environment. Most medico-legal issues in general practice do not arise from rare clinical errors, but from common gaps---poor documentation, missed follow-up, communication failures, and guideline deviation.
This is where AI tools, when used wisely, can quietly reduce risk in day-to-day practice.
Documentation: the first line of legal defense
In medico-legal cases, "if it is not documented, it did not happen." AI-based ambient scribes and smart EHR assistants help create structured, timestamped notes during the consultation. They reduce missed details like red flag symptoms, counselling given, or safety-net advice. Better notes mean clearer clinical reasoning, which is critical when records are reviewed months or years later.
Clinical decision support at the point of care
Modern AI decision-support tools embedded in EHRs prompt differential diagnoses, highlight guideline-based investigations, and flag high-risk symptoms. In family practice, this is especially useful for chest pain, fever, abdominal pain, and chronic disease reviews. These prompts do not replace judgment, but they reduce the risk of "you did not consider" allegations, which are common in litigation.
Medication safety and prescribing errors
AI-driven prescription checks can flag drug--drug interactions, renal dose adjustments, duplicate therapies, and allergy conflicts in real time. Many medico-legal claims in primary care involve adverse drug events. Consistent use of AI checks strengthens prescribing defensibility.
Follow up and test result tracking
Missed lab reports and delayed follow up are classic legal traps. AI enabled task management systems can track abnormal results, generate alerts, and document patient notifications. This creates a clear audit trail showing reasonable systems were in place.
Communication and patient understanding
AI tools can generate visit summaries in simple language, improving patient understanding and adherence. Clear communication reduces complaints and disputes.
In summary, AI in family practice is not about automation hype. It is about safer systems---better notes, better follow-up, and better clinical consistency. Used as an assistive layer, AI can quietly lower medico-legal risk while letting us focus on the human side of care.
Dr. Syed Mubarak
MBBS, PGDFM, PBDGM
Project Director- Health & Wellbeing, Bosch Global Software

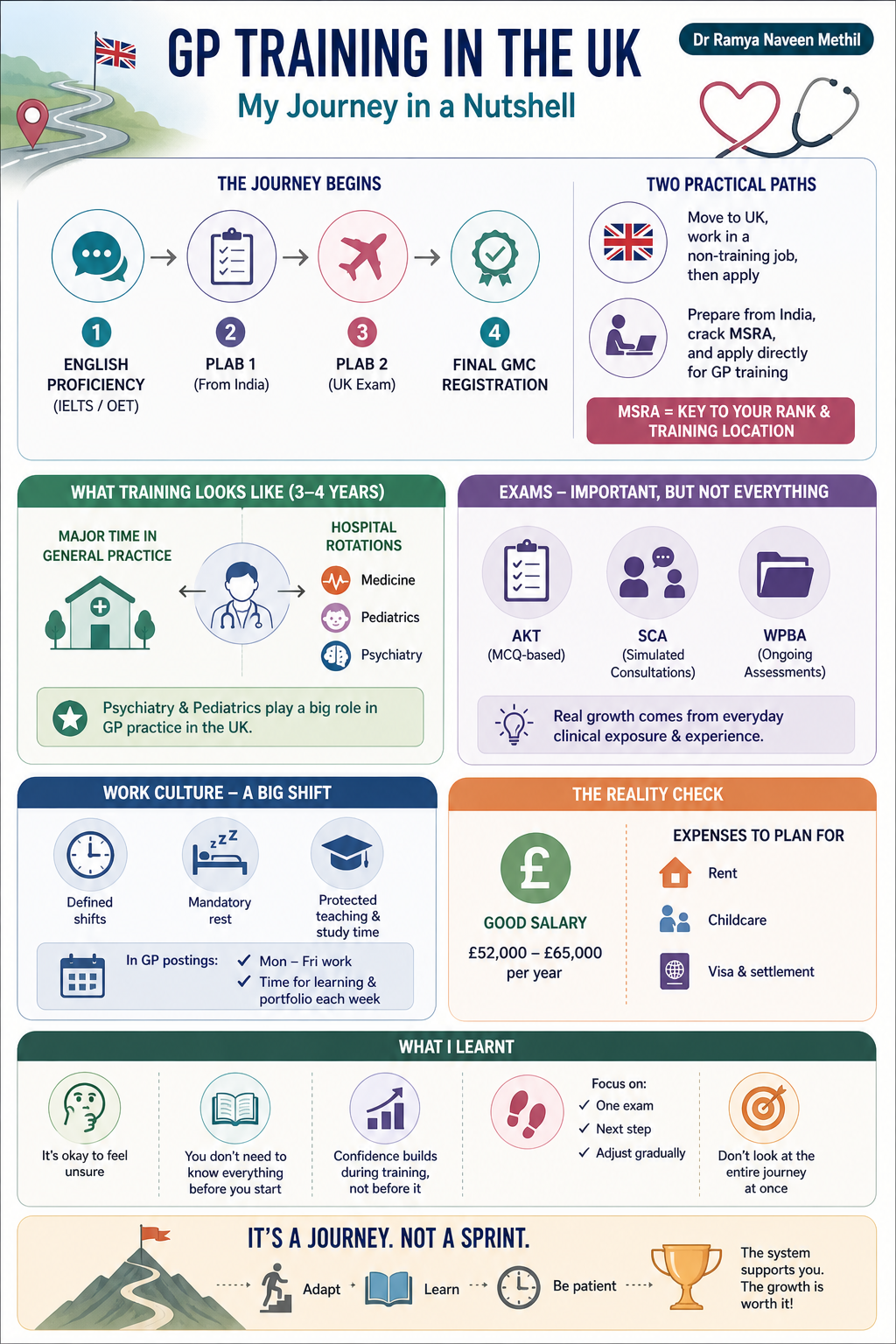
GP Training in the UK: A Practical Overview
Dr. Ramya Naveen Methil
When I first started exploring GP training in the UK, it felt overwhelming. Too many steps, too many exams, and a lot of uncertainty. But once I broke it down and took it one step at a time, it became much more manageable---and definitely achievable.
The journey essentially begins with getting your GMC registration. For that, you'll need:
- English proficiency (IELTS/OET)
- PLAB 1 & 2
- GMC registration
PLAB 1 can be done from India, but PLAB 2 requires travel to the UK. That's usually the first big transition point for most of us.
Once registered, you have two practical options:
- Move to the UK, start in a non-training job, and then apply
- Or prepare from India, write the MSRA exam, and directly apply for GP training
The MSRA is now the key step---it decides your ranking and largely determines where you train.
What training actually feels like
GP training lasts 3--4 years, and it's a mix of:
- General practice (major portion)
- Hospital rotations (medicine, pediatrics, psychiatry, etc.)
What really stood out was how important psychiatry and pediatrics are. In the UK, GPs manage a large part of these cases themselves, especially in early stages. That was quite different from my experience in India---and initially a bit intimidating---but incredibly useful in the long run.
Exams --- but not the whole story
You will need to clear:
- AKT (MCQ-based)
- SCA (simulated consultations)
- WPBA (ongoing assessments)
But honestly, what shapes you more than exams is day-to-day clinical exposure---how you communicate, document, and think through cases.
Work culture --- a big shift
One of the biggest differences is the work structure:
- Defined shifts (no 24--36 hour duties)
- Mandatory rest between shifts
- Protected teaching and study time
Once you move into GP postings, it's mostly:
- Monday to Friday work
- Some time each week dedicated to learning or portfolio work
It takes time to adjust---but it's a healthier system overall.
The reality check
Financially, GP training is reasonably well paid:
- Around £52,000--£65,000 per year
But expenses matter:
- Rent is the biggest cost
- Childcare can be expensive
- Visa and settlement costs add up
So planning ahead financially is important.
What I learnt through the journey
- It's okay to feel unsure in the beginning
- You don't need to know everything before you start
- Confidence builds during training---not before it
Most importantly: Don't look at the entire journey at once.
Just focus on:
- Clearing one exam
- Taking the next step
- Adjusting gradually
This is not the easiest path---but it is a structured and achievable one.
If you're willing to adapt, learn, and stay patient with the process, the system will support you, and the growth is worth it.

Reflections from Practice - Gratification Comes - Sometimes very late, But surely..!
Dr.Priti Shankar, Afpi Secretary
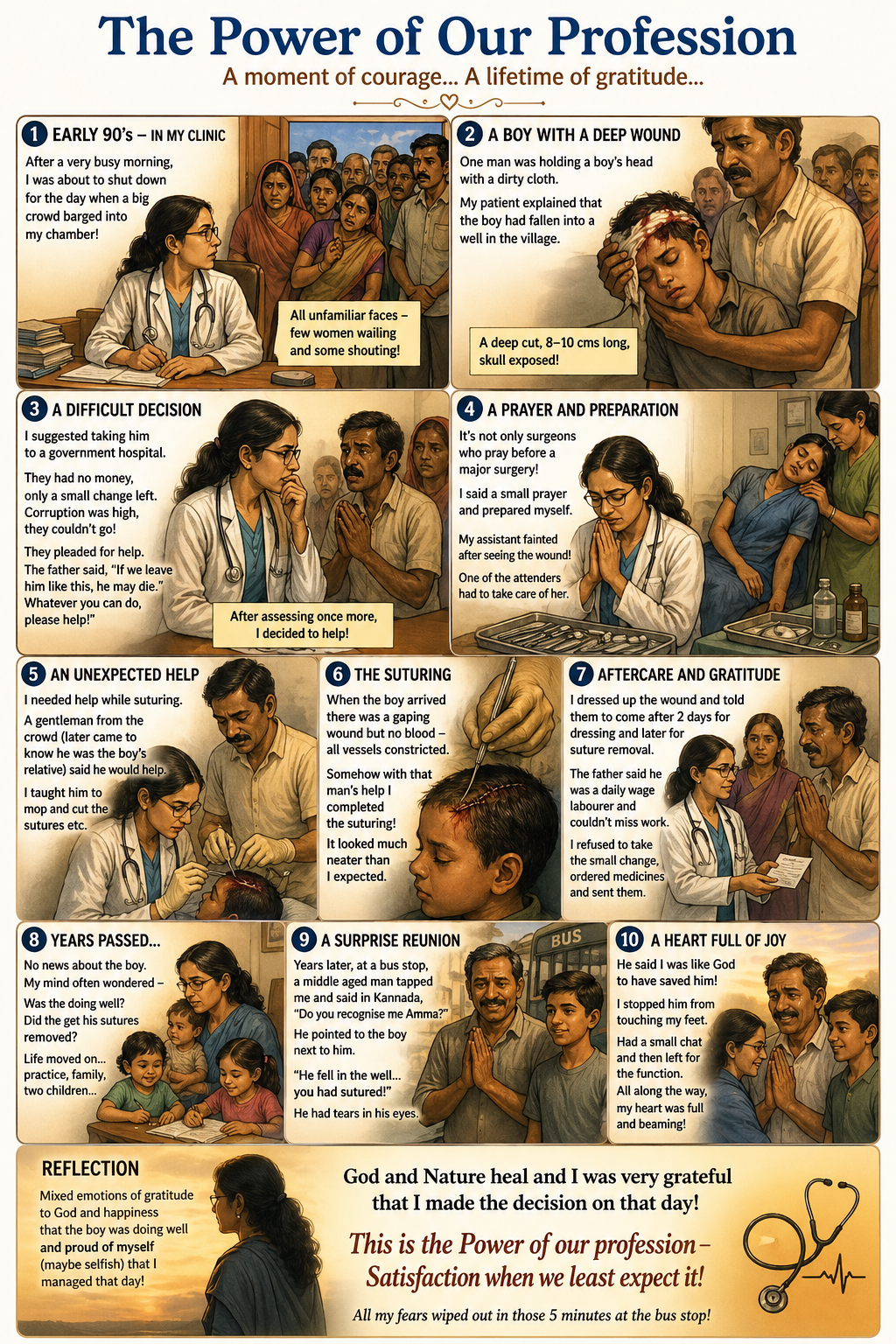
This was in the early 90's about 5/6 years into my practice in my clinic!
One afternoon after a very busy morning (because other clinics were closed due to festival) was about to shutdown for the day when a big crowd barged into my chamber! Initial reaction was apprehension ! All unfamiliar faces -few women wailing and some shouting! Before I could react one of my patients who stayed close to my clinic hushed the others and started talking (much to my relief).
One man in the crowd was holding a 8 to 9 years boy's head with a cloth which was far from clean ( dirty by all standards).
My patient explained that the boy had fallen into a well in the village and they had taken a bus and come to my patients home for help.
I looked at the wound 8 to 10 cms long a deep cut with the skull exposed !
All my neighbours and other patients knew that I do suturing of wounds and minor procedures.
But this was too much for me so I suggested to take the boy to a government hospital.
They said they had no money only a small change left.
Those days corruption at the hospitals was at the peak so they couldn't take to the hospital!
They didn't even have sufficient auto fare.
The relatives of the boy started crying and pleading for me to do something!The father said if we leave him like this he may die so whatever you can do please help!
They said we can't take him anywhere else without money!
I was known in the neighborhood to waive off the fees sometimes!
After assessing the situation once more I decided to help!
It's not only surgeons who pray before a major surgery! This was truly major for me .I was terrified and nervous initially but said a small prayer and with the blessings from God I proceeded after taking all the equipment ready!
Things were not going to be smooth as my clinic assistant almost fainted after seeing the wound!
One of the attenders had to give her water and take care of her .
Now I needed help while suturing and as I looked around a gentleman from the crowd ( later came to know he was boy's relative) said he would help.
I was hesitant but with no other choice left I taught him to mop and cut the sutures etc.
When the boy arrived there was a gaping wound but no blood!
All vessels constricted.
Somehow with that man's help I completed the suturing!
I least expected it to look as neat as it actually did, much to my surprise. I dressed up the wound and told the parents to bring him again for dressing etc after 2 days and later for suture removal!
The father started crying and said he was a labourer on daily wages and he can't miss work and come.
I refused to take the small change he was paying me and ordered antibiotics and pain killers from the nearby chemist and sent them.
I heaved a big sigh of relief and had mixed emotions as they left!
Days passed, months passed and any enquiry from my other patients about the boy was fruitless.
My mind often in a turmoil whether the boy was doing well did he get sutures removed.
As I got engrossed in my practice and family with 2 children one toddler and one about 7 years the incident was pushed away from my forefront memory!
Those days telephone communication was not very easy only trunk calls !
Years later I was waiting at the bus stop for an auto to go to a social function with my in laws!
My mother in law waiting at the function!
One middle aged man tapped me from behind and said in Kannada "Do you recognise me Amma"
I am from Tamilnadu and my Kannada was just enough to understand him !
I said " Illa theriya illa"
Both Tamil and Kannada mix!
Then he pointed out to the a 15/16 year old boy next to him and said " Ivan gotthithiya - Do you remember or know him"
I again said Illa theriya illa.
He pointed out to that boy's head and said he had fallen in the well and you had sutured!
"Adhe huduga "
He had tears in his eyes and was very emotional and said you are like God to have saved him !
He was falling at my feet which I stopped him from doing.
Had a small conversation with him asking about the boys studies etc and then had to leave.
On the other side my mother in law eagerly waiting for me !
So I caught the 5th auto and left for the function.
All along the way to the function my heart was full and beaming!
Mixed emotions of gratitude to God and happiness that the boy was doing well and proud of myself (maybe selfish) that I managed that day!
The whole incident again flashed back of my assistant fainting and I had goosebumps!
God and Nature heal and I was very grateful that I made the decision on that day!
This is the Power of our profession - Satisfaction when we least expect it !
All my fears wiped out in those 5 minutes at the bus stop,!
God is the Healer and we are mere instruments!!
💰 Smart Financial Planning for Family Physicians – Dr. Uma Madavachetty

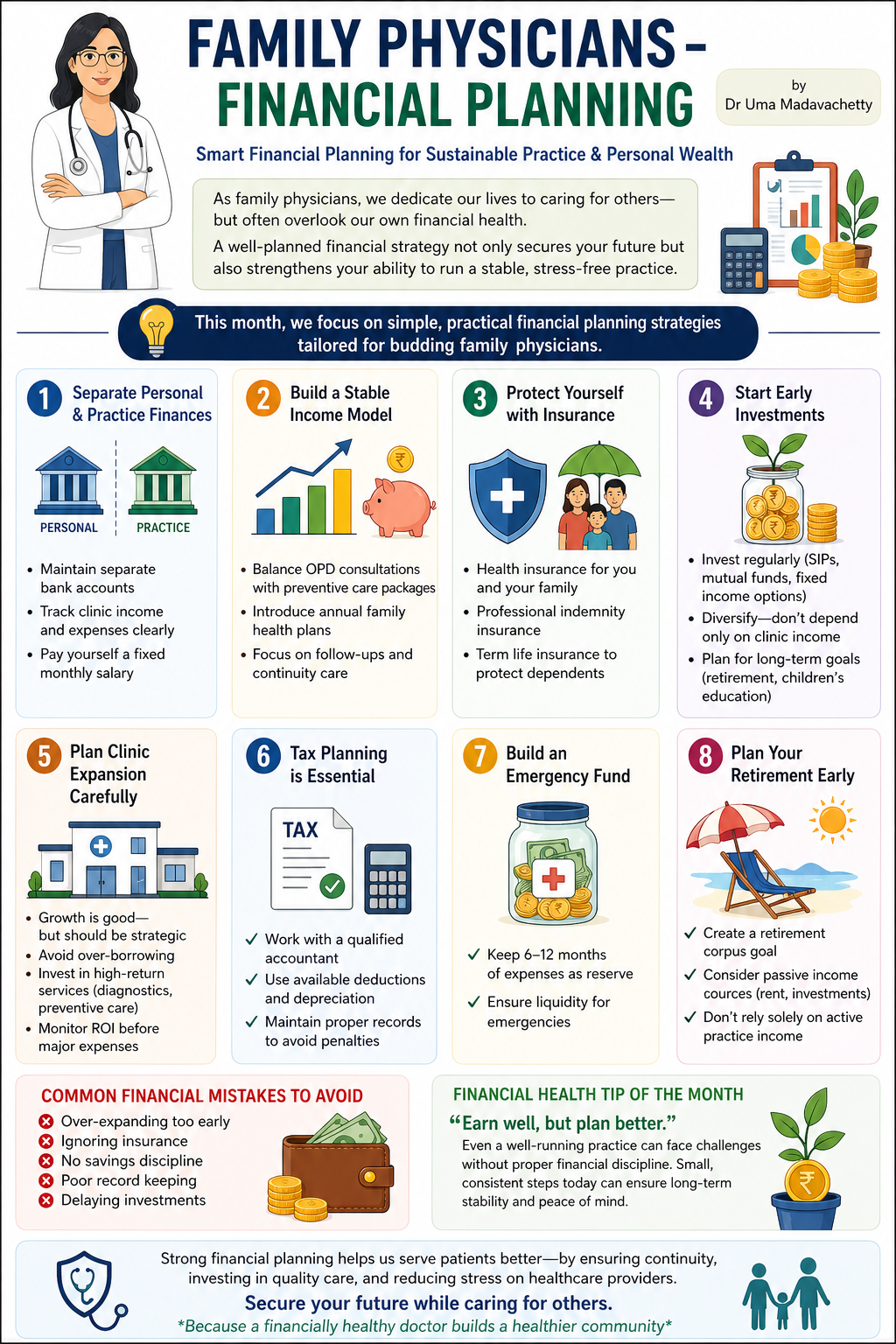
FAMILY PHYSICIANS- Financial planning
Dr. Uma Madavachetty
Smart Financial Planning for Sustainable Practice & Personal Wealth
As family physicians, we dedicate our lives to caring for others---but often overlook our own financial health.
A well-planned financial strategy not only secures your future but also strengthens your ability to run a stable, stress-free practice.
This month, we focus on simple, practical financial planning strategies tailored for budding family physicians
1. Separate Personal & Practice Finances
Mixing finances is one of the most common mistakes.
Maintain separate bank accounts
Track clinic income and expenses clearly
Pay yourself a fixed monthly salary
Build a Stable Income Model
Family practice income can fluctuate.
Balance OPD consultations with preventive care packages
Introduce annual family health plans
Focus on follow-ups and continuity care
2. Protect Yourself with Insurance
Your income depends on your health
Health insurance for you and your family
Professional indemnity insurance
Term life insurance to protect dependents
3. Start Early Investments
Avoid delaying wealth creation.
Invest regularly (SIPs, mutual funds, fixed income options)
Diversify---don't depend only on clinic income
Plan for long-term goals (retirement, children's education)
4. Plan Clinic Expansion Carefully
Growth is good---but should be strategic.
Avoid over-borrowing
Invest in high-return services (diagnostics, preventive care)
Monitor ROI before major expenses
5. Tax Planning is Essential
Smart tax planning increases net income.
Work with a qualified accountant
Use available deductions and depreciation
Maintain proper records to avoid penalties
6. Build an Emergency Fund
Unexpected situations can affect both personal and clinic finances.
✔ Keep 6--12 months of expenses as reserve
✔ Ensure liquidity for emergencies
7. Plan Your Retirement Early
Medical professionals often delay retirement planning.
Create a retirement corpus goal
Consider passive income sources (rent, investments)
Don't rely solely on active practice income
Common Financial Mistakes to Avoid: Over-expanding too early, Ignoring insurance, No savings discipline, Poor record keeping, Delaying investments
Financial Health Tip of the Month: "Earn well, but plan better. Even a well-running practice can face challenges without proper financial discipline. Small, consistent steps today can ensure long-term stability and peace of mind."
Strong financial planning helps us serve patients better---by ensuring continuity, investing in quality care, and reducing stress on healthcare providers.
Secure your future while caring for others. Because a financially healthy doctor builds a healthier community
⚖️ MEDICO-LEGAL OPD CASES -- WHAT WENT WRONG?
A middle-aged patient came with chest discomfort and mild sweating. Doctor diagnosed acidity, gave antacids, and sent home. No ECG or cardiac evaluation was done. Patient later suffered myocardial infarction. Legal principle aligned with: Jacob Mathew vs State of Punjab.
What was NOT done: No basic investigation (ECG), no risk stratification, no documentation of ruling out cardiac cause.
Legal POV: Court checks: *Would a reasonable doctor have done an ECG?* → Yes. Failure to rule out life-threatening condition = negligence.
Key - "Error of judgment is allowed---but failure to take basic precautions is not."
Patient with mild fever/URI given multiple drugs (antibiotic + NSAID + others) without clear indication. Developed severe drug reaction (e.g., SJS).
What was NOT done: No clear indication for antibiotic, no documentation of reasoning, no warning about drug risks.
Legal POV: Prescribing without indication = breach of standard care. If harm occurs → direct liability. "Patient insisted" is not a defense.
Key - "Unnecessary treatment that causes harm is negligence."
Doctor evaluated patient correctly and gave appropriate treatment. However, no written notes of history/exam/advice were recorded. Patient later alleged wrong treatment.
What was NOT done: No documentation of history/exam, no record of advice or follow-up instructions.
Legal POV: Courts rely on records, not recollection. Absence of documentation = presumption against doctor.
Key - "If it is not documented, it is considered not done."
🌟 DOCTOR IN SPOTLIGHT: DR. SWAPNA BHASKAR

From Fragile beginnings to Fearless journeys : My Life in Family Medicine
Dr Swapna Bhaskar, MBBS, DNB (Family medicine), PGDMCH, FRACGP
Consultant GP - Plaza Medical Centre, Kalgoorlie , Western Australia
Former HOD Family Medicine, St Philomena's Hospital, Bangalore, India. Former President - AFPI Karnataka.
" You are a smart young efficient doctor, why waste your career doing DNB Family Medicine ?" " What is family medicine and its scope for doctors like you" " Aren't you wasting your time and career by choosing a non existent speciality with no clarity on your future " These were a few questions that kept coming my way multiple times from well-wishing elders ,teachers, and friends during my post graduation and early years as a family physician. I am certain these are thoughts that cross the minds of many young doctors in the field of Family Medicine. Chapter 1 - Uncertainty, Sustainability, and the Courage to Continue With dreams of specializing in Internal Medicine or Ophthalmology, I landed in Bangalore as a young mother in 1999. Not wanting my son to be reared by a caretaker, I was mostly a "stay-at-home mom" for four years, spending only a few hours with a local pediatrician as his clinical assistant. Many of my friends were specialists and had set up busy practices by then. Determined to become a specialist, I tried and miserably failed multiple entrances, finally managing to borderline pass the NBE one.
After a hospital based test and interview, I was elated to be among the shortlisted candidates. The receptionist at the office then gave us the backdoor information that the Gen Medicine seat was already given to an internal candidate, and graciously offered the opportunity of joining a new field called "Family Medicine". This would train you primarily in internal medicine, along with other subjects she mentioned. In my confused state, it seemed like a pretty good deal, becoming a specialist without having to battle more entrance exams. So, without much choice I became a "Family Medicine" trainee by chance! We were proudly (and somewhat nervously) the first batch to take on this then unknown three year speciality training in Bangalore, though a few senior doctors had already secured the degree through an exit exam.
Being a PG felt like an endless grind, looking forward to the day it would finally be done.! The most intimidating part of our training was the uncertainty. Neither the faculty nor my three peers knew what we were expected to learn or teach, where we should be posted, what our roles were in those postings, how the final exams would be structured, or what future opportunities awaited us. We were routinely used to fill gaps across departments under the pretext of needing training in all departments. .Despite the lack of overt recognition, Family Medicine doctors slowly proved themselves to be an indispensable part of the hospital when required
Through those three grueling years, I found myself on the verge of quitting my training more times than I can count.. Giving up on my training would have meant letting down my family, whose encouragement gave me the strength to persevere. In the middle of that, we also welcomed our second child. Amid the struggle, one saving grace was my medical director's promise of a faculty position, a flicker of light at the end of the tunnel. That assured my journey would not be in vain.
Gradually, the challenges of training brought clarity and confidence. I became equipped to provide care across all ages, organ systems, and genders, going beyond the narrow focus of many specialised PGs.. The difficulties of handling patients and relatives, doing procedures, communicating with patients while balancing work, family and finance made me a really strong and competent family doctor by then.
Passing the DNB exams remains an enigma to me even now. Yet it marked a turning point, enabling me to become one of the first Family medicine qualified faculty to establish a department which was all this while led by Internal Medicine and Community Medicine specialists. The first few months were the usual OP/IP routine. Then I slowly started what we never had during my training: actual teaching for Family Medicine PGs As the department expanded, I had the good fortune of working with some wonderfully energetic bunch of peers who helped build the department with pride. I watched my students flourish in many directions within Family Medicine, some building successful clinics of their own, some dedicating themselves to teaching, and others pursuing sub-specialties such as Infectious Diseases, Transitional Care, and Palliative Care During my initial two years, I also started a small evening general practice clinic near home, with minimal investment, mainly to improve my difficult financial situation. I began with just a small room and a waiting area, quietly hoping that at least 3--4 patients would walk in to see a new, inexperienced doctor. There was no grand inauguration, no newspaper advertisements, and no marketing team, just quiet determination. I did not take a single holiday, ensuring no patient would return unattended. Gradually, patients began to trust my care, and word-of-mouth became my most powerful form of publicity. Soon, I started receiving referrals from general practitioners and specialists in the area, all while maintaining ethical practice without compromise.
Life moved on with its share of highs and lows, while I continued to do my best,often imperfectly but sincerely, as daughter, sister, wife, mother, teacher, and Family Doctor.
Although I reckoned I knew what family medicine was, my entry into the Academy of Family Physicians of India around 2015 changed many perspectives about this wonderful field. Here I got a chance to work and interact with esteemed faculty of Vellore CMC, GPs from America, UK, Australia and many other countries. Holding the position of the Karnataka chapter President for 3 years gave me the opportunity to host the National conference, state conferences, and collaborate with esteemed organisations like NTI, Niti Aayog , State health Department, RGUHS to name a few. AFPI became an important catalyst in my growth, giving me the opportunity to take on dynamic roles such as DNB examiner, thesis evaluator, and OSCE preparation team member. My heart swelled with pride whenever I shared my speciality with family, friends, and well-wishers who had earlier doubted my choice. A special mention to my guru, Dr B C Rao, a guiding father figure whose energetic and inspiring presence always reminded me of my potential, and who always made me believe I was capable of achieving and envisioning.
Here I was, heading a department and the AFPI state chapter, sculpting many family physicians, spearheading activities related to health education, medical education and primary care of a country which needs it! I am extremely proud of what I achieved in those 16 years, and I thank God for the CHANCE given to me, depriving me of my CHOICES. Still, something within me felt missing, and I knew I needed to explore further.
Hearing from some undergraduate friends about how highly valued GPs were abroad gradually planted the idea of stepping out of my comfort zone. I also grew curious about how training and medical practice might differ in a developed country. But a lingering question remained... Was it still possible at my age?
August 2023 - the page of RACGP president Michael wright
Chapter 2: When dreams beckon midway and change your path. In 2022, I took a tough yet crucial decision to migrate to Australia. Why Australia? Maybe it was my friends already working there as GPs, the chance to skip the hospital route and go straight into general practice, less lawsuits against doctors, or even the better pay, honestly, there wasn't one clear reason. After clearing a few exams, completing numerous documents, and nothing to lose, my husband and I landed in Kalgoorlie, a small town in Western Australia with a population of about 30,000, smaller than even a few crossroads in Bangalore. Leaving behind my boys, parents, lovely friends, colleagues, and important responsibilities, I once again landed in uncertainty, which, looking back, felt almost funny in its irony.
I found myself back in student mode after 18 years, learning the Australian approach to general practice, as well as new cultures, guidelines, music, dance, sports, cuisine, and much more. In those two years, the thought of quitting crossed my mind again a dozen times, weighed down by endless assessments, paperwork, and supervision demands. But perseverance paid off, and seeing my name in the FRACGP register last year was a moment I had only ever dreamed of. In this small town today, I am known for the care I provide.
A four-year-old calling out "That's my doctor" in a crowded supermarket, a salesperson going the extra mile to find me the perfect shade of paint, or an 80-year-old arriving with a homemade cake to celebrate my fellowship, these simple moments mean more than words can express. Looking back, across all the places I've been and the challenges I've faced, I realize this journey was never just about degrees or achievements. It was about growing, starting over, and learning how to truly care for people.
As words often attributed to Theodore Roosevelt remind us: "No one cares how much you know until they know how much you care." And in the end, that is what I believe matters the most.



🧩 FUN CORNER & CLINICAL ENGAGEMENT
THE DETECTIVE HAT- "What Would You Do Next?"
CASE 1 -- Persistent Fever
A 30-year-old with fever for 4 days, mild headache, platelets 1.3 lakh, WBC slightly low, vitals stable, no focus.
Best next step?
A. Start antibiotics
B. Start antivirals
C. Observe + repeat labs + warning signs
D. Admit immediately
CASE 2 -- Borderline UTI Symptoms
A 28-year-old female with mild burning urination, no fever, no flank pain, symptoms since 1 day.
What would you do?
A. Start antibiotics immediately
B. Encourage fluids + observe
C. Urine culture first, then treat
D. Start IV antibiotics
CASE 3 -- Subclinical Hypothyroidism
A 38-year-old female, TSH = 8, normal T3/T4, mild fatigue.
Best approach?
A. Start high-dose thyroxine
B. Start low-dose thyroxine
C. Observe + repeat TSH in 6--8 weeks
D. Ignore completely
# ANSWER: C | B | C
Clinical Pearls
Case 1: Viral patterns (dengue-like) → don't jump to antibiotics
Case 2: Very early mild symptoms → can observe before labeling UTI
Case 3: Not all TSH elevations need treatment immediately
ECG Case: A 48-year-old male presents with intermittent palpitations. No syncope. Vitals stable.
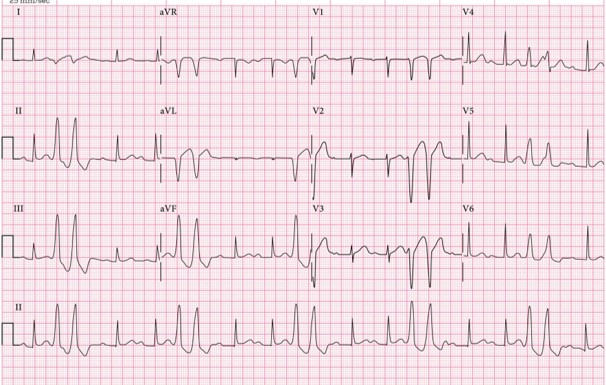
1. What is the rhythm abnormality?
2. Which ECG feature helped you identify it?
3. Is this benign or potentially serious?
4. What is your first-line management in OPD?
How to Diagnose: Look for these 4 clues:
1. Two consecutive early beats → that's why it's a couplet
2. Wide, bizarre QRS complexes (>120 ms, abnormal shape)
3. No preceding P wave (confirms ventricular origin)
4. Compensatory pause after the pair
Differentiate from: NSVT (≥3 beats), SVT with aberrancy.
2 beats = couplet ; ≥3 beats = think VT
Why couplets matter more than single PVCs: Higher arrhythmogenic potential, can progress to VT, more concerning if frequent / symptomatic / structural heart disease.
Treatment Approach: If asymptomatic + normal heart → Reassure, lifestyle advice. If symptomatic → Beta-blocker: Metoprolol 25--50 mg OD. Red flags (syncope, known CAD, frequent couplets) → Echo, Holter, electrolytes, refer cardiology.
X-ray – What is your diagnosis?
Look for a bright white (radio-opaque) density along the urinary tract path. Trace from kidney → ureter → bladder. Correlate with pain side and symptoms. Keep in mind: Calcium stones usually visible; Uric acid stones often NOT seen on X-ray.

Spondylolisthesis case: A patient presents with chronic low back pain ± radicular symptoms.
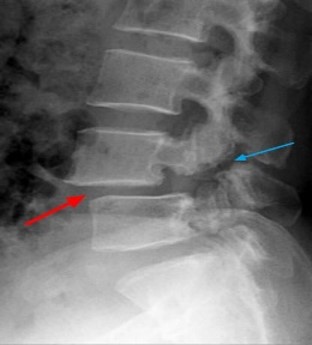
Answers:
1. Diagnosis: Forward slip of one vertebra over another (commonly L5 over S1).
2. Grading (Meyerding): Grade 1: <25%, Grade 2: 25-50%, Grade 3: 50-75%, Grade 4: >75%.
3. Who can be managed in OPD: Grade 1-2, no neurological deficit, mild to moderate pain → analgesics, core strengthening, activity modification.
4. When to ask for MRI: radicular pain, neurological deficit, suspected nerve compression, no improvement after 4-6 weeks. Red flags: motor weakness, bladder/bowel symptoms, progressive signs → immediate referral + MRI.
🎲 Ending Insight
 Figure 31: Snake and Ladder
Figure 31: Snake and Ladder Snakes & Ladders: The Journey of Clinical Practice
Practice In Family Medicine Is Like Snakes & Ladders --- Every Step Matters.
Contact the editor for any queries or suggestions: doctoraminaa@gmail.com